


Abstract
Background:Tinnitus and hearing loss are both prevalent chronic conditions that can significantly impair quality of life. While prior studies have explored the association between tinnitus and mortality, many have failed to isolate the effect of tinnitus from that of coexisting hearing loss—a frequent comorbidity—which may have introduced confounding and biased the results.
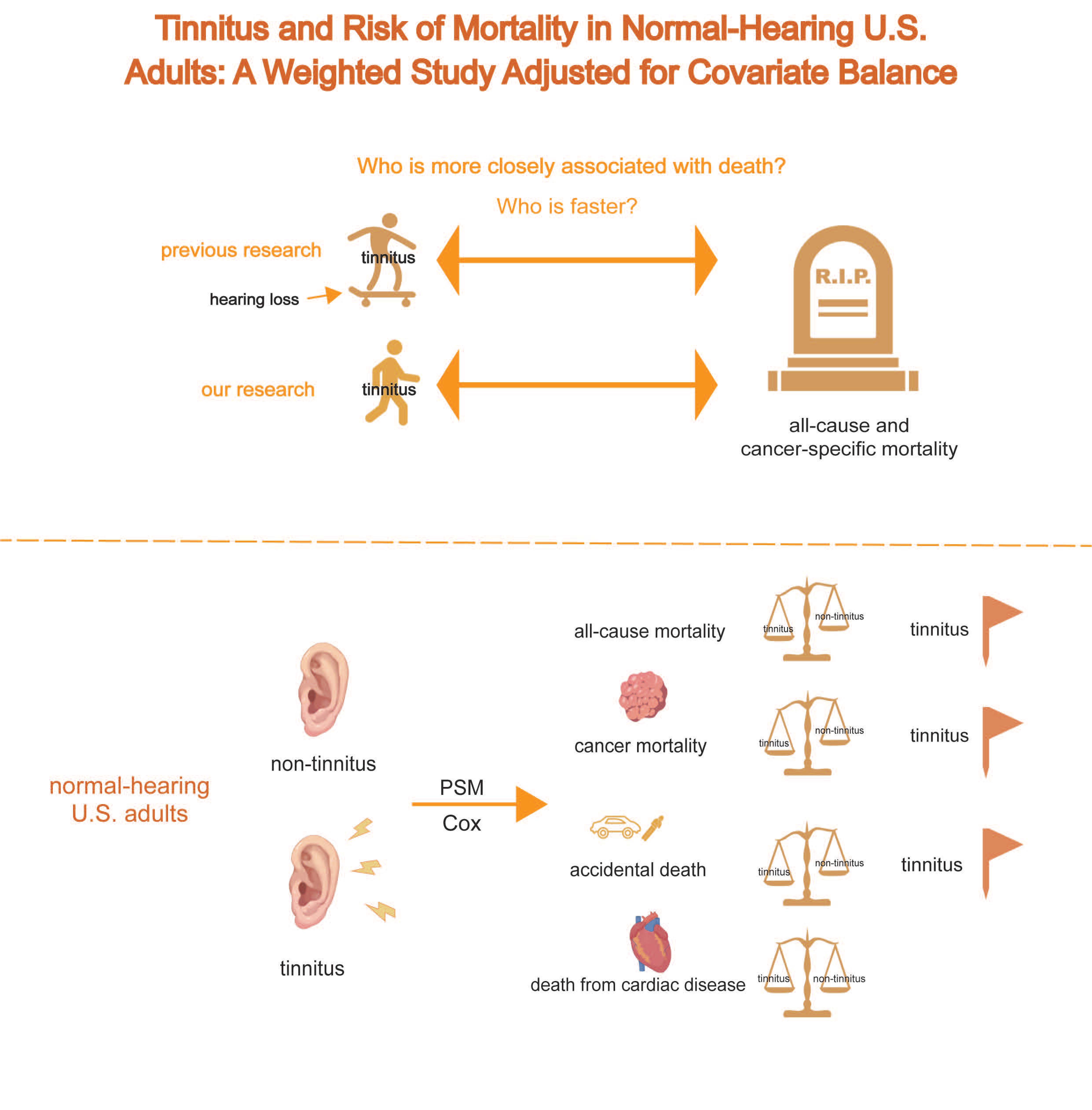
Objectives:To investigate the association between tinnitus and both all-cause and cause-specific mortality among U.S. adults aged 20-69 years with normal hearing.
Design and Methods:We conducted a population-based cross-sectional analysis using data from five cycles of the National Health and Nutrition Examination Survey. Adults aged 20-69 years with audiometrically confirmed normal hearing were included. Tinnitus status was self-reported. Key covariates included demographic characteristics, comorbid conditions etc.We implemented propensity score matching and multivariable-adjusted Cox proportional hazards models to estimate the hazard ratios (HRs) for all-cause and cause-specific mortality.
Results:Tinnitus was found to be significantly associated with an increased risk of all-cause mortality (HR: 1.84; 95% CI: 1.38-2.44). A particularly elevated risk was observed for cancer-specific mortality (HR: 2.11; 95% CI: 1.26-3.58). Importantly, these findings persisted after adjusting for multiple covariates in the matched cohort, highlighting the robustness of the results derived from a balanced comparison.
Conclusions:Among U.S. adults with normal hearing, tinnitus was independently associated with increased risks of all-cause and cancer-specific mortality. These findings underscore the importance of recognizing tinnitus as not merely a benign symptom, but a potential marker of broader health risks, even in individuals without hearing impairment.
Keywords: tinnitus; mortality; balance; normal hearing; National Health and Nutrition Examination Survey (NHANES)
Introduction
Tinnitus is characterized by the perception of sound in the absence of an identifiable external source and is widely recognized as both a somatic and psychological symptom that may signal underlying health disturbances [1] . Due to the clinical heterogeneity of tinnitus in terms of etiology and symptoms, as well as a series of accompanying symptoms such as insomnia, irritability, depression, anxiety, hearing difficulties, and hearing allergies [1,2] , patients who visit the hospital with tinnitus as their chief complaint may be biased from the actual tinnitus population. But according to the results of most current studies, the rate of tinnitus is 10-15%, which increases with age [3-5] .
Tinnitus, as a highly prevalent and widely symptomatic disease, can cause a huge burden on patients and affect their lives, and the probability of tinnitus patients requiring disability pension is far more than normal people, also causing a huge burden on socioeconomic [6] . Although most patients with tinnitus are able to cope with the distress caused by tinnitus, a subset of patients believe that tinnitus has severely affected their lives [3] . Damage to any part of the hearing pathway can lead to tinnitus, as can some non-hearing disorders [7] , so there is currently no appropriate therapy for tinnitus due to the complexity of its pathogenesis [1] . In addition, research has elaborated that tinnitus is a risk factor for depression [8,9] , cardiovascular disease [10] , cognitive disorders [11] , glaucoma [12] , and other diseases, which illustrates that tinnitus may affect the organism more severely than we thought. The most frequent comorbid symptom among tinnitus sufferers is hearing loss.
Hearing loss is an extremely prevalent accompanying symptom in the patients with tinnitus [13] , and the vast majority of patients with tinnitus have varying degrees of hearing loss, but some researchers have found that approximately one-third of people with tinnitus have hearing thresholds within normal range [14] . Hearing loss has an effect on all-cause and cause-specific mortality in patients, and the exclusion of hearing loss as a confounding bias is necessary when examining the relationship between whether a patient has tinnitus and mortality [15] . In terms of pathology, hearing loss leads to significant white matter changes, and white matter changes are considered to be one of the manifestations of tinnitus. White matter integrity in patients with chronic tinnitus is both directly affected by age and mediated by hearing loss [16] .
The development of hearing loss negatively affects higher auditory processing abilities, and when hearing problems other than hearing loss are present, individuals with normal hearing may have increased compensatory attentional resource mobilisation, as opposed to individuals with hearing loss who show a loss of compensatory network connectivity involving multisensory integration [17] . From the molecular biology point of view, studies have identified tinnitus as a distinct disorder independent of hearing difficulties [18] .
Historically, this phenomenon has been largely overlooked in research, resulting in insufficient consideration of hearing loss—a common comorbid symptom of tinnitus—in studies investigating the association between tinnitus and other health outcomes. This omission may have introduced potential bias into previous findings. To minimize such confounding effects, the present study exclusively included participants with tinnitus who demonstrated normal hearing function.
In several past studies, investigators have found that, in addition to hearing related factors [19] , obesity [20] , smoking [21] , gender [22] , mental stress [3,23] , hyperlipidemia [24] , and cardiovascular disease [25] are risk factors for tinnitus. Considering the above, tinnitus appears to be intricately linked with various systemic conditions, exerting health effects that may extend beyond current understanding.
To gain deeper insights into the relationship between tinnitus and broader health outcomes, as well as its potential prognostic implications, we sought to eliminate the confounding influence of hearing loss. Therefore, this study specifically focused on individuals with tinnitus and normal hearing to assess its association with all-cause and cause-specific mortality. Our findings aim to inform targeted screening and management strategies for this unique patient population in clinical settings.
Methods
Study Population
Participants in this study were derived from the National Health and Nutrition Examination Survey (NHANES) (https://www.cdc.gov/nchs/ ), an ongoing program designed to assess the health and nutritional status of a nationally representative sample of the U.S. population. NHANES employs a continuous, multistage, stratified probability sampling design across 2-year cycles, initiated in 1999 and approved by the National Center for Health Statistics Institutional Review Board.
We utilized data from five survey cycles (1999-2004, 2011-2012, and 2015-2016), selecting those that provided complete information on tinnitus-related variables as well as relevant covariates. All data—encompassing demographic, socioeconomic, and health interview responses, audiometric assessments, and laboratory test results—were collected by trained health professionals according to standardized protocols. Appropriate sample weights, as recommended in the official NHANES documentation, were applied to ensure nationally representative estimates during statistical analyses.
To reduce age-related confounding and improve cognitive assessment consistency, we restricted our analytic sample to adults aged 20 to 69 years, thereby excluding individuals whose cognitive function may not have fully developed (young adults) or may have declined due to aging (older adults). The study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. As the analysis was based on publicly available, de-identified NHANES datasets, it was deemed exempt from institutional review board oversight and did not require individual informed consent.
Through December 31, 2019, the National Center for Health Statistics supplied mortality statistics connected to the National Death Index. The underlying cause of death was classified following the International Classification of Diseases, 10th Revision (ICD-10). Cardiac disease mortality was defined as death from cardiac disease (ICD-10 codes I00-I09, I11, I13, and I20-I51), while cancer mortality was classified as malignant neoplasms (ICD-10 codes C00-C97). The follow-up duration was calculated as the number of months from the date of completion of the tinnitus questionnaire to the date of death or until December 31, 2019, whichever occurred first. To minimize the potential impact of reverse causality, individuals who died within the first 24 months of follow-up were excluded from the analysis.
Through questionnaire surveys, an assessment was made of the existence and severity of tinnitus. The steps for selecting patients with tinnitus have been used in many literatures [26,27] . Tinnitus was classified as present or absent based on a yes or no answer to the following questions, “In the past 12 months, have you ever had ringing, roaring, or buzzing in your ears?”/ “In the past 12 months, have you been bothered by ringing, roaring, or buzzing in your ears or head that lasts for 5 minutes or more?”.
To exclude the impact of hearing on tinnitus, we limited our study to tinnitus patients with normal hearing. Selection steps for patients with normal hearing have also been verified [28] . Low frequency hearing loss (LFHL) was defined by the pure-tone average (PTA) of hearing thresholds at 500, 1000, and 2000 Hz, speech frequency hearing loss (SFHL) by the PTA of hearing thresholds at 500, 1000, 2000, and 4000 Hz, and high frequency hearing loss (HFHL) by the PTA of hearing thresholds at 3000, 4000, 6000, and 8000 Hz. According to the World Health Organization criteria, normal hearing was defined as an unassisted PTA of less than 25 dB in the better hearing ear. We included data from participants who had normal hearing at all three frequencies.
In terms of covariates, only age was reported as a continuous variable. NHANES reported any poverty income ratio (PIR) higher than 5 as 5. Self-reported sociodemographic characteristics were described in the following categories: sex (male/female), race/ethnicity (non-Hispanic white, non-Hispanic black, and Hispanic or other), marital status (married, never married or living with partner, divorced or separated, and widowed), education level (less than high school, high school or equivalent, and college or above), and family income (PIR: <1.30, 1.30-3.49, or ≥3.5). Using measured height and weight, we worked out balance (yes, no), body mass index (BMI) and classified it into three categories (<25, 25-30, ≥30). Lifestyle behaviors such as smoking history (former, never, and now), drinking history (mild, moderate, heavy, former, and never), and physical activity (total metabolic equivalent <450, 450-749.9, ≥750) were also variables of interest. In addition, we recorded the presence or absence of the following diseases at any time during the participant's lifetime: congestive heart failure (CHF), hypertension, diabetes mellitus (DM), coronary cardiac disease, stroke, heart attack, hyperlipidemia, and cancer.
Statistical Analysis
In accordance with the analysis guidelines of the NHANES, we performed all analyses with the use of sample weights, stratification, and clustering with a complex sampling design to account for sampling bias. In the final included normal hearing population with complete data, the continuous variables were described by MD (SD), and the categorical variables were described by the total number of subjects (weighted percentage), using Chi-square independent test and one-way analysis of variance, respectively. The propensity score matching and cox regression model adjusted for all factors were used to analyze the correlation between the existence or absence of tinnitus and mortality. In the propensity score analysis, cox regression was used to build a model to estimate the presence of tinnitus by the following variables: age, sex, race/ethnicity, marital status, education level, PIR, balance, BMI, smoking, drinking, physical activity, CHF, hypertension, DM, coronary heart disease, stroke, heart attack, hyperlipidemia, and cancer. The matching cohorts of tinnitus users and non-tinnitus users were established using 2:1 matching with 0.05 caliper distance and the nearest neighbor matching algorithm without displacement. Standardized mean differences (SMD) and p-values were calculated for all included variables to assess balance between the matched cohort of individuals with tinnitus and the cohort without tinnitus. Cox regression analysis was adjusted for all variables to estimate the hazard ratio (HR) and 95% confidence interval (CI) between tinnitus and mortality in the unmatched and matched cohorts, respectively. Individuals with a pertinent medical background for the outcome of each examined condition were excluded in the cause-specific mortality study (eg, cancer mortality excluded previously diagnosed cancer).
In addition, stratified analyses and interaction analyses were performed to check if there were differences in the associations between different age, sex, PIR, BMI, physical activity, and smoking status. All analyses were conducted based on R (version 4.1.3), and a p-value less than 0.05 was considered statistically significant.
Results
Participants Characteristics
The process of participant selection is illustrated in Figure 1. Among the 24,718 individuals who completed the tinnitus questionnaire across the selected NHANES cycles, 21,480 were between 20 and 69 years of age. After excluding participants with abnormal hearing thresholds, missing data on key covariates or mortality outcomes, and those who died within the first 24 months of follow-up, a final analytic cohort of 3,869 participants with normal hearing was established. Table 1 showed the demographic and clinically relevant data of the cohort. The tinnitus group had a higher mean (SD) age (38.88 [0.43] years vs 38.02 [0.27] years) and a higher proportion of men (42.47% [301] vs 43.75% [1266] ) than the non-tinnitus group. Individuals with tinnitus exhibited lower levels of physical activity and higher smoking rates compared to those without tinnitus. Additionally, they had a higher prevalence of hypertension, hyperlipidemia, and stroke. After applying propensity score matching, a well-balanced cohort of individuals with and without tinnitus was created (Table 1 ).
Figure 1. Flowchart of this study.
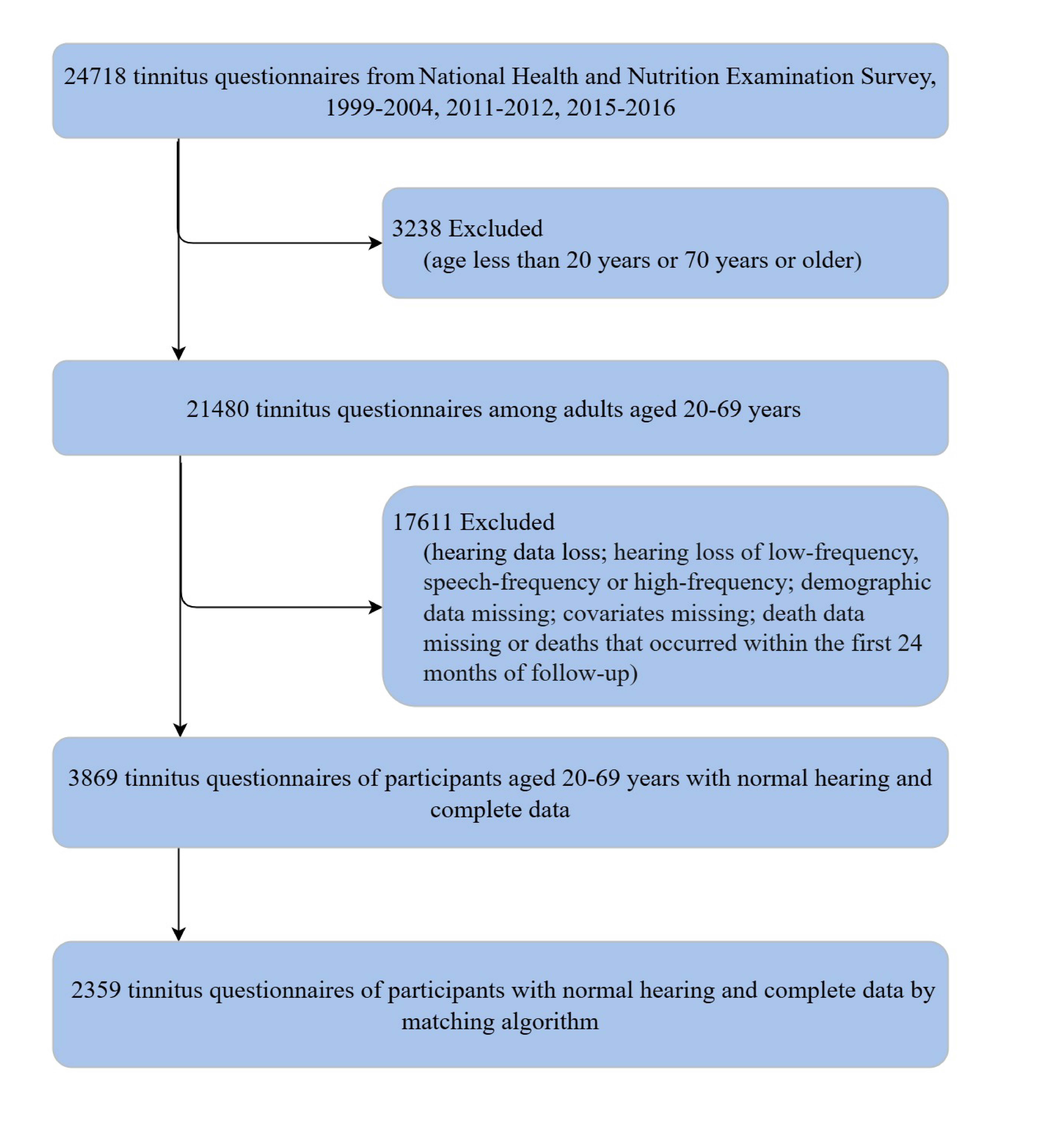
Table 1. Baseline characteristics of tinnitus in subjects with normal hearing
|
Unmatched |
|
Matched |
|
|||
|
variable |
No tinnitus |
Tinnitus |
P value |
No tinnitus |
Tinnitus |
P value |
|
Respondents, No. |
3058 |
811 |
|
1556 |
803 |
|
|
Balance |
|
|
0.07 |
|
|
0.91 |
|
yes |
185(5.13) |
63(7.37) |
|
122(6.26) |
60(7.14) |
|
|
no |
583(21.86) |
150(20.96) |
|
301(22.15) |
150(21.15) |
|
|
not record |
2290(73.01) |
598(71.67) |
|
1133(71.58) |
593(71.71) |
|
|
Age, mean (SD) |
38.02(0.27) |
38.88(0.43) |
0.06 |
38.65(0.35) |
38.80(0.42) |
0.79 |
|
Sex |
|
|
0.5 |
|
|
0.42 |
|
Female |
1792(56.25) |
510(57.53) |
|
902(55.44) |
504(57.54) |
|
|
Male |
1266(43.75) |
301(42.47) |
|
654(44.56) |
299(42.46) |
|
|
Race and ethnicity |
|
|
< 0.0001 |
|
|
0.89 |
|
Hispanic or other |
1022(21.17) |
256(16.22) |
|
441(16.54) |
255(16.36) |
|
|
Non-Hispanic Black |
706(12.79) |
148( 9.33) |
|
305(9.89) |
146(9.29) |
|
|
Non-Hispanic White |
1330(66.04) |
407(74.44) |
|
810(73.56) |
402(74.35) |
|
|
Marriage status |
|
|
0.21 |
|
|
0.96 |
|
divorced or separated |
328(10.60) |
114(13.66) |
|
190(11.90) |
110(13.38) |
|
|
married |
1644(54.91) |
407(52.51) |
|
827(53.94) |
405(52.67) |
|
|
never married/living with partner |
902(28.68) |
241(27.59) |
|
450(28.45) |
239(27.66) |
|
|
widowed |
60(1.36) |
22(1.89) |
|
36(1.63) |
22(1.91) |
|
|
not recorded |
124(4.44) |
27(4.34) |
|
53(4.08) |
27(4.38) |
|
|
Educational level |
|
|
0.23 |
|
|
0.92 |
|
college or above |
1578(60.45) |
421(58.18) |
|
796(59.18) |
418(58.22) |
|
|
high school or equivalent |
1191(35.38) |
319(38.45) |
|
625(37.17) |
315(38.39) |
|
|
less than high school |
289(4.18) |
71(3.36) |
|
135(3.65) |
70(3.39) |
|
|
PIR |
|
|
0.03 |
|
|
0.83 |
|
<1.3 |
748(18.61) |
228(23.41) |
|
418(20.66) |
221(22.73) |
|
|
1.3-3.49 |
1287(39.18) |
329(37.37) |
|
632(39.45) |
328(37.69) |
|
|
≥3.5 |
1023(42.20) |
254(39.23) |
|
506(39.89) |
254(39.58) |
|
|
BMI |
|
|
0.1 |
|
|
0.73 |
|
<25 |
1020(37.47) |
289(39.49) |
|
529(38.29) |
285(39.18) |
|
|
25-30 |
1076(33.47) |
245(28.14) |
|
506(30.97) |
245(28.40) |
|
|
≥30 |
962(29.07) |
277(32.36) |
|
521(30.74) |
273(32.42) |
|
|
Physical activity |
|
|
0.74 |
|
|
0.81 |
|
<450 |
1293(43.60) |
351(45.23) |
|
710(46.84) |
348(45.24) |
|
|
450-749.9 |
1123(33.22) |
287(32.87) |
|
527(31.04) |
282(32.67) |
|
|
≥750 |
642(23.18) |
173(21.90) |
|
319(22.13) |
173(22.10) |
|
|
Smoke |
|
|
0.01 |
|
|
0.9 |
|
former |
554(19.35) |
183(22.11) |
|
317(20.99) |
181(22.26) |
|
|
never |
1795(55.39) |
391(46.47) |
|
810(48.56) |
391(46.89) |
|
|
now |
709(25.26) |
237(31.42) |
|
429(30.45) |
231(30.85) |
|
|
Alcohol use |
|
|
0.002 |
|
|
0.72 |
|
former |
392(10.81) |
133(13.53) |
|
234(12.56) |
130(13.51) |
|
|
never |
446(12.47) |
83( 8.87) |
|
196(10.64) |
83( 8.95) |
|
|
now |
2034(71.37) |
568(75.32) |
|
1075(74.02) |
563(75.25) |
|
|
not record |
186(5.35) |
27(2.28) |
|
51(2.78) |
27(2.30) |
|
|
Congestive heart failure |
|
|
0.04 |
|
|
0.4 |
|
no |
3037(99.51) |
799(98.57) |
|
1544(99.59) |
795(99.00) |
|
|
yes |
21(0.49) |
12(1.43) |
|
12(0.41) |
8(1.00) |
|
|
Hypertension |
|
|
0.22 |
|
|
0.87 |
|
no |
2292(76.26) |
573(73.99) |
|
1135(74.96) |
569(73.99) |
|
|
yes |
766(23.74) |
238(26.01) |
|
421(25.04) |
234(26.01) |
|
|
DM |
|
|
0.03 |
|
|
0.73 |
|
yes |
186(4.57) |
64(6.29) |
|
117(5.57) |
60(6.05) |
|
|
no |
2572(92.46) |
684(92.06) |
|
1311(92.22) |
680(92.29) |
|
|
not record |
300(2.96) |
63(1.65) |
|
128(2.21) |
63(1.66) |
|
|
coronary.heart.disease |
|
|
0.57 |
|
|
0.75 |
|
no |
3035(99.21) |
799(98.92) |
|
1546(99.32) |
791(98.91) |
|
|
yes |
23(0.79) |
12(1.08) |
|
10(0.68) |
12(1.09) |
|
|
Hyperlipidemia |
|
|
0.85 |
|
|
0.83 |
|
no |
1061(35.33) |
269(34.90) |
|
522(34.94) |
266(34.85) |
|
|
yes |
1997(64.67) |
542(65.10) |
|
1034(65.06) |
537(65.15) |
|
|
Stroke |
|
|
0.1 |
|
|
0.38 |
|
no |
3031(98.99) |
795(98.20) |
|
1539(98.82) |
788(98.35) |
|
|
yes |
27(1.01) |
16(1.80) |
|
17(1.18) |
15(1.65) |
|
|
Heart attack |
|
|
0.12 |
|
|
0.79 |
|
no |
3028(99.00) |
796(98.26) |
|
1538(98.76) |
789(98.33) |
|
|
yes |
30(1.00) |
15(1.74) |
|
18(1.24) |
14(1.67) |
|
|
Cancer |
|
|
0.03 |
|
|
0.53 |
|
no |
2947(95.62) |
758(92.86) |
|
1482(94.59) |
752(93.05) |
|
|
yes |
111(4.38) |
53(7.14) |
|
74(5.41) |
51(6.95) |
|
Abbreviations: NA, not applicable; SMD, standardized mean difference; PIR, poverty income ratio; BMI, body mass index; DM, diabetes mellitus.
Tinnitus and Mortality
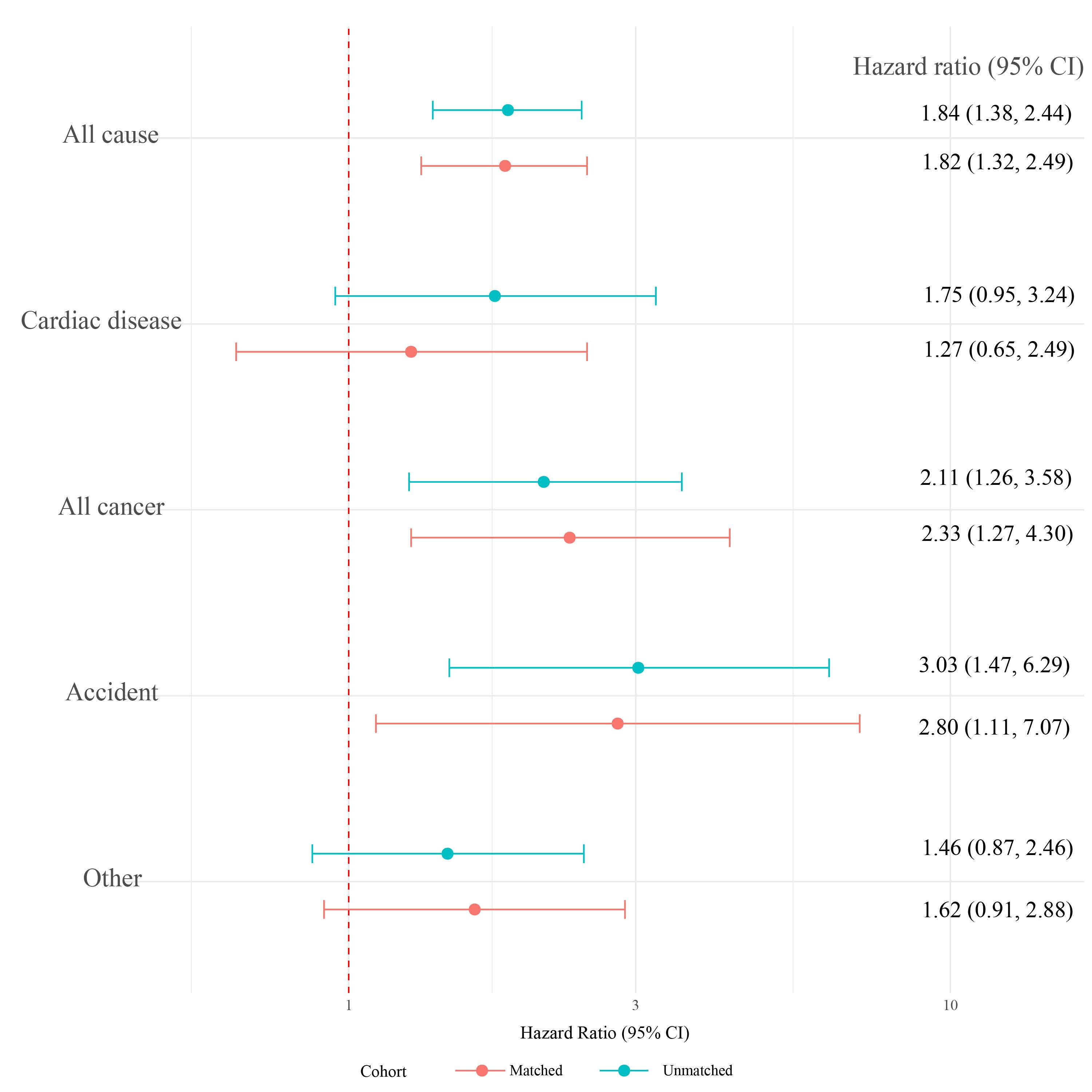
As shown in Figure 2, subjects with tinnitus an increased chance of dying from all causes and from cancer. After adjustment for demographic characteristics, lifestyle, and chronic diseases, compared with those without tinnitus, the HR for all-cause mortality was 1.84(95% CI, 1.38 to 2.44) in the unmatched cohort and 1.82(95% CI, 1.32 to 2.49) in the matched cohort. The HR for cancer mortality were 2.11 (95% CI, 1.26 to 3.58) and 2.33 (95% CI, 1.27 to 4.30), respectively. As can be seen, these associations were more significant in the cohort after matching. In addition, tinnitus was linked to a higher risk of accidental death (unmatched cohort: HR, 3.03; 95%CI, 1.47-6.29; matched cohort: HR, 2.80; 95% CI, 1.11-7.07) and death from other causes (unmatched cohort: HR, 1.46; 95% CI, 0.87-2.46; matched cohort: HR, 1.62; 95% CI, 0.91-2.88). In contrast, tinnitus did not affect the probability of death from cardiac disease (unmatched cohort: HR, 1.75; 95%CI, 0.95-3.24; matched cohort: HR, 1.27; 95% CI, 0.65-2.49).
Figure 2. Adjusted Hazard Ratios of all-cause and cause-specific mortality comparing tinnitus with no tinnitus, National Health and Nutrition Examination Survey, 1999-2004, 2011-2012, 2015-2016.
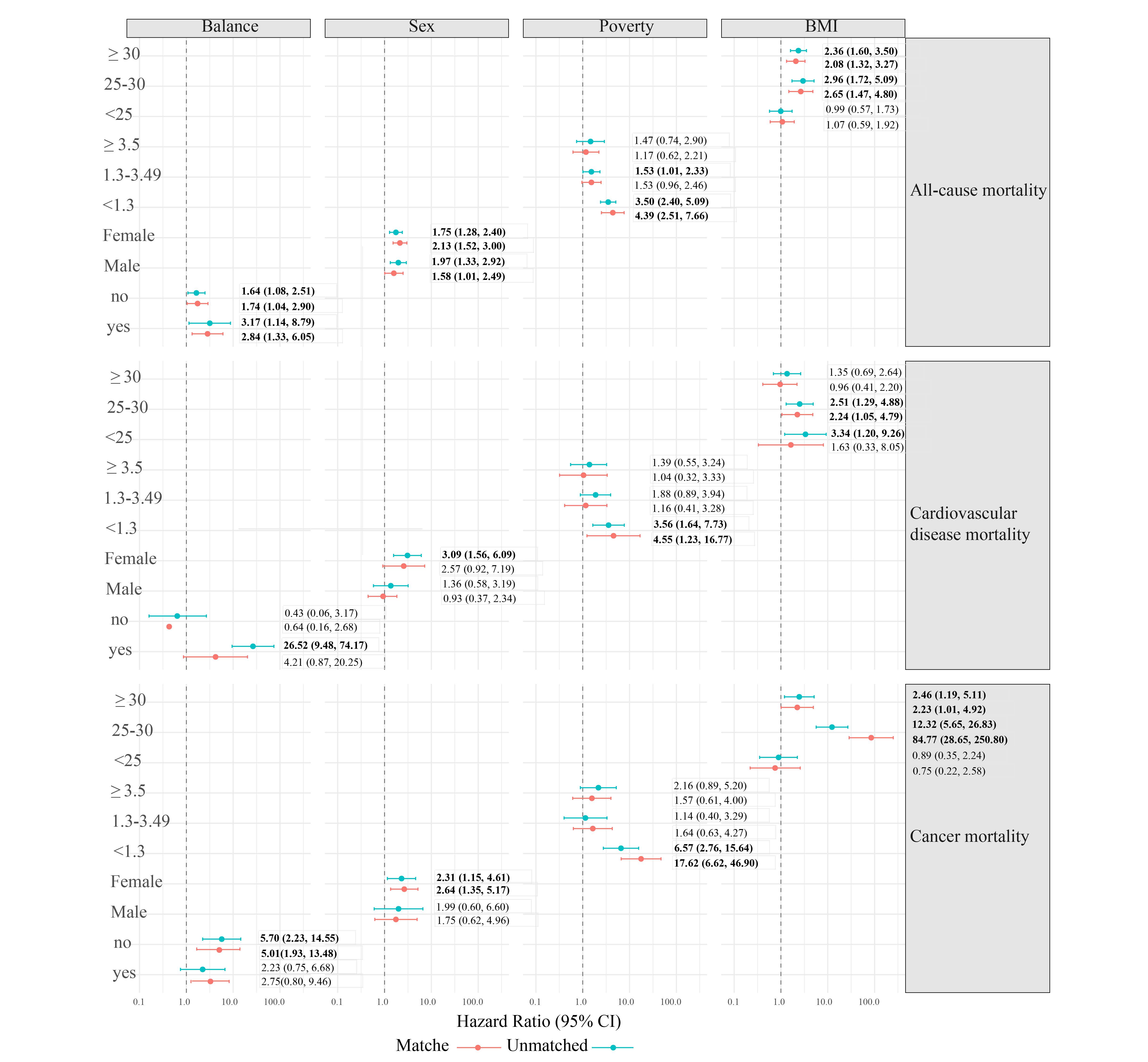
Most subgroups retained these connections. The correlation between tinnitus and all-cause mortality was stronger among participants with a BMI ≥ 30 (unmatched cohort: HR, 2.36; 95%CI, 1.60-3.50; matched cohort: HR, 2.08; 95% CI, 1.32-3.27) and BMI 25-30 (unmatched cohort: HR, 2.96; 95%CI, 1.72-5.09; matched cohort: HR, 2.65; 95% CI, 1.47-4.80) (Figure 3). The association between tinnitus and cancer mortality was stronger among people with no balance (unmatched cohort: HR, 5.70; 95%CI, 2.23-14.55; matched cohort: HR, 5.01; 95% CI, 1.93-13.48) and female (unmatched cohort: HR, 2.31; 95%CI, 1.15-4.61; matched cohort: HR, 2.64; 95% CI, 1.35-5.17) (Figure 3).
Figure 3. Stratified Hazard Ratios and 95% CIs for all-cause and cause-specific mortality according to tinnitus.
Discussion
This study investigated the relationship between tinnitus and its associated risk factors, as well as the impact of tinnitus on mortality from various diseases. The findings offer valuable insights for the clinical screening and management of tinnitus patients with normal hearing.
In this national representative US adult cohort study, we observed that subjects with tinnitus had a higher rate of dying from all causes and cancer, and accidental death, but tinnitus did not affect the rate of death from cardiac disease. In the course of subgroup analysis, we found that the relevance between tinnitus and all-cause mortality was greater in participants with a BMI ≥30 and 25-30. The correlation between tinnitus and cancer mortality was stronger in female and people with no balance.
Tinnitus, one of the three major otologic challenges, has been closely associated with increased suicide rates in many countries [1,29] . Therefore, the screening and therapy of patients with tinnitus is particularly important. The main symptoms of drug ototoxicity are tinnitus, hearing loss and balance disorders [31] . The relationship between hearing loss, balance disorders and all-cause and cause-specific mortality has been systematically addressed in studies [32,33] . Research on the relationship between tinnitus and all-cause and cause-specific mortality is still in a blank state.
In addition, it has been shown that hearing loss is related to an elevated risk of all-cause and cause-specific mortality [32] , and a study by Martz E et al. found that those with tinnitus had lower cause-specific mortality than those without tinnitus, but it did not control for the confounding factor of hearing loss [34] . To eliminate the effect of hearing loss on tinnitus, this study compared tinnitus with all-cause and cause-specific mortality only in the normal hearing population.
Tinnitus patients have deteriorated neuropsychological ability and lower sense of social identity, which affects socialization, decision-making and work ability, which in turn leads to a higher risk of death [35-37] . In terms of neuropsychological regulation, clinical studies have shown that tinnitus patients exhibit signs of impaired the hypothalamic–pituitary–adrenal axis (HPA axis) and higher levels of mental stress compared to non-tinnitus patients [38-40] . The deterioration of the ability to relax and activate the parasympathetic nervous system in individuals with tinnitus can have some negative physical and psychological effects [41] , such as dysregulation of the body's stress system, depression, and sleep disturbances, all of which are related with an elevated risk of death [42] .
From the perspective of social identity, some studies have found that due to the persistence of tinnitus, patients' sleep quality also can be impacted, which affects their social activities and productivity [43] . In addition, for people in some professions such as musicians, the impact of tinnitus on their careers is tremendous. Tinnitus may make them incompetent for work and their sense of social identity declines so rapidly that they are more likely to end up in demoralization or even suicide [44] .
Therefore, while treating tinnitus, we need to pay attention to patients' mental health issues and provide them with the necessary psychological guidance and support. We should provide comprehensive treatment to help patients return to a healthy state and improve their quality of life and social identity.
Patients with tinnitus have a higher risk of death from cancer than those without tinnitus. On the one hand, cancer patients become anxious or even depressed because of cancer, and anxiety and depression can in turn trigger or aggravate tinnitus [45] . Therefore, patients with tinnitus indicate higher levels of anxiety and depression, and both anxiety and depression and tinnitus itself put cancer patients at higher risk of death [46] .
On the other hand, ototoxicity can also cause tinnitus. Ototoxicity caused by cancer chemotherapy drugs such as cisplatin and vincristine can have a detrimental effect on quality of life [47] . Patients develop a fear of social life and of worsening tinnitus. Patients with mild and moderate-severe tinnitus fear that chemotherapy with drugs such as cisplatin will further aggravate the symptoms of tinnitus and thus become skeptical or even refuse drug treatment for cancer [48] .
In this study, the correlation between tinnitus and all-cause mortality was stronger in participants with a BMI ≥30 and 25-30. Although the underlying mechanisms between tinnitus and mortality are not known, several causes can be considered. First, tinnitus may interact with psychosocial factors in patients and is associated with poor health outcomes, including cognitive deficits, decrease in social activities, mental health impairment [49,50] , and reducing ability to perform activities of daily living. Obese populations may be more inclined to reduce necessary activities, which further exacerbates the harm caused by obesity to the organism. Second, the study by Wade, K. H. indicated a causal relationship between higher BMI and all-cause and cause-specific mortality [51] . In addition, it has also been shown that weight loss after diet and physical activity interventions relieved tinnitus symptoms and improved quality of life in tinnitus sufferers [52,53] . Combined with this study, we can speculate that perhaps maintaining an appropriate BMI has a positive effect on reducing both tinnitus morbidity and mortality, which provides new ideas for managing diet and physical activity in tinnitus patients.
The correlation between tinnitus and cancer mortality is stronger in women. During chemotherapy in cancer patients, estrogen levels are higher in women compared to men and fluctuate significantly with environmental factors and the menstrual cycle. Fluctuations in estrogen levels may lead to vasodilatory dysfunction [54] , which may affect the blood supply to the inner ear and aggravate tinnitus. In addition, estrogen level change may mediate chemotherapeutic drug resistance [55] and promote cancer disease progression [56] leading to increased cancer mortality.
Cancer patients without balance have increased risk of falls compared to the rest of the population. On the one hand, people who suffer from balance disorders and tinnitus have a greater fear of falling and reduce their daily activities [57,58] , thereby increasing the risk of cancer [59] , all of which increase the risk of death [60] . On the other hand, in patients with neurological cancers, balance disorders may be a sequela of the cancer itself or secondary to treatment [61] . As neurological cancer patients deteriorate, the metabolism of fluid in the inner ear [62] , which leads to labyrinthine disorders, results in severe balance disorders, tinnitus, etc. Tinnitus is also a marker of further deterioration of neurological cancer in patients with balance disorders [63] . The correlation between tinnitus and cancer mortality is stronger in those without balance.
Strengths and limitations
A major strength of this study is the exploration of the relationship between tinnitus and all-cause and cause-specific mortality only in a normal hearing population, which eliminated the effect of hearing loss on tinnitus. Second, this study uses a large, representative sample of NHANES, a research program that is prospective and based on enrollment to obtain high-quality information. Third, the application of propensity score matching (PSM) analysis to adjust for important demographic variables is also an advantage of this study. Considering the significant disparities in the number of tinnitus and non-tinnitus couples, PSM reduces the effects of bias and confounding variables in the study to allow reasonable comparisons between the matched cohort of individuals with tinnitus and the cohort without tinnitus. Last but not least, subgroup analyses of gender, marital status, and education level were conducted to address the issue of heterogeneity in this study.
There are still some limitations in our study. First, because the study was observational, the causal relationship between the presence of tinnitus and the severity of tinnitus and all-cause and cause-specific mortality could not be determined. Second, although we adjusted for confounders as much as possible, there may still be some confounders that we did not take into account. Third, our study population was US adults between the ages of 20 and 69, and the findings may not be applicable to children and older adults >69 years of age.
Future studies should evaluate the mechanisms that link tinnitus with total and cause-specific mortality in order to individualize the treatment of tinnitus patients with normal hearing, thereby improving the quality of life and reducing mortality in tinnitus patients.
Conclusion
Among U.S. adults with normal hearing, tinnitus was independently associated with increased risks of all-cause and cancer-specific mortality. By employing propensity score matching to ensure covariate balance, this study enhances the validity of the observed associations and reduces the influence of potential confounders. These findings underscore the importance of recognizing tinnitus as not merely a benign symptom, but a potential marker of broader health risks, even in individuals without hearing impairment. Clinicians and public health professionals should consider systematic evaluation and follow-up in this population, particularly focusing on mental health, cancer screening, and accident prevention. Future research is needed to elucidate the underlying mechanisms of the association between tinnitus and mortality in participants with normal hearing and to explore the relationship between tinnitus severity and mortality in people with normal hearing.
Abbrevations
SD: standard deviation; HR: hazard ratio; 95%CI: 95%confidence interval; NHANES: National Health and Nutrition Examination Survey; STROBE: Strengthening Reporting of Observational Studies in Epidemiology; ICD-10: International Classification of Diseases, 10th Revision; LFHL: Low frequency hearing loss; PTA: pure-tone average; Hz: hertz; SFHL: speech frequency hearing loss; HFHL: high frequency hearing loss; dB: decibel; PIR: poverty income ratio; BMI: body mass index; CHF: congestive heart failure; DM: diabetes mellitus; MD: mean deviation; SMD: standardized mean differences; eg: exempli gratia; Vs: versus; HPA axis: hypothalamic–pituitary–adrenal axis; PSM: propensity score matching; NA, not applicable.
Declarations
Author Contributions
Yuchen Zhang: Conceptualization, Software; Yanqiang Zhang: Methodology; Data curation; Ziyue Fu: Writing-Original draft; Kaile Wu, Yehai Liu: Software, Validation; Chuanlu Shen: Writing- Reviewing and Editing.
Acknowledgements
Not applicable.
Ethics Approval and Consent to Participate
NHANES was approved by the National Center for Health Statistics Research Ethics Review Board, and consent from all participants was documented. All methods were performed in accordance with the relevant guidelines and regulations of NHANES.
Funding Information
The study was supported by funding from the National Natural Science Foundation of China [Grant No. 82371133].
Competing Interests
The authors declare that they have no existing or potential commercial or financial relationships that could create a conflict of interest at the time of conducting this study.
Data Availability
All data needed to evaluate the conclusions in the paper are present in the paper or the Supplementary Materials. Additional data related to this paper may be requested from the authors.
References
[1] Baguley D, McFerran D, Hall D. (2013) Tinnitus. Lancet (London, England).382(9904):1600-7 https://doi.org/10.1016/s0140-6736(13)60142-7.
[2] Langguth B, Kreuzer PM, Kleinjung T, De Ridder D. (2013) Tinnitus: causes and clinical management. The Lancet Neurology.12(9):920-30 https://doi.org/10.1016/s1474-4422(13)70160-1.
[3] Sharma A, Sood N, Munjal S, Panda N. (2021) Perception of Tinnitus Handicap And Stress Across Age Groups in Normal Hearing. The international tinnitus journal.25(1):13-7 https://doi.org/10.5935/0946-5448.2020004.
[4] Tunkel DE, Bauer CA, Sun GH, Rosenfeld RM, Chandrasekhar SS, Cunningham ER, Jr., et al. (2014) Clinical practice guideline: tinnitus. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery.151(2 Suppl):S1-s40 https://doi.org/10.1177/0194599814545325.
[5] Jafari Z, Kolb BE, Mohajerani MH. (2019) Age-related hearing loss and tinnitus, dementia risk, and auditory amplification outcomes. Ageing research reviews.56:100963 https://doi.org/10.1016/j.arr.2019.100963.
[6] Friberg E, Jansson C, Mittendorfer-Rutz E, Rosenhall U, Alexanderson K. (2012) Sickness absence due to otoaudiological diagnoses and risk of disability pension: a nationwide Swedish prospective cohort study. PloS one.7(1):e29966 https://doi.org/10.1371/journal.pone.0029966.
[7] Esmaili AA, Renton J. (2018) A review of tinnitus. Australian journal of general practice.47(4):205-8 https://doi.org/10.31128/ajgp-12-17-4420.
[8] Choi J, Lee CH, Kim SY. (2021) Association of Tinnitus with Depression in a Normal Hearing Population. Medicina (Kaunas, Lithuania).57(2) https://doi.org/10.3390/medicina57020114.
[9] Granjeiro RC, Kehrle HM, de Oliveira TS, Sampaio AL, de Oliveira CA. (2013) Is the degree of discomfort caused by tinnitus in normal-hearing individuals correlated with psychiatric disorders? Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery.148(4):658-63 https://doi.org/10.1177/0194599812473554.
[10] Huang YS, Koo M, Chen JC, Hwang JH. (2017) The association between tinnitus and the risk of ischemic cerebrovascular disease in young and middle-aged patients: A secondary case-control analysis of a nationwide, population-based health claims database. PloS one.12(11):e0187474 https://doi.org/10.1371/journal.pone.0187474.
[11] Chu HT, Liang CS, Yeh TC, Hu LY, Yang AC, Tsai SJ, et al. (2020) Tinnitus and risk of Alzheimer's and Parkinson's disease: a retrospective nationwide population-based cohort study. Scientific reports.10(1):12134 https://doi.org/10.1038/s41598-020-69243-0.
[12] Loiselle AR, Neustaeter A, de Kleine E, van Dijk P, Jansonius NM. (2020) Associations between tinnitus and glaucoma suggest a common mechanism: A clinical and population-based study. Hearing research.386:107862 https://doi.org/10.1016/j.heares.2019.107862.
[13] Hoare DJ, Edmondson-Jones M, Sereda M, Akeroyd MA, Hall D. (2014) Amplification with hearing aids for patients with tinnitus and co-existing hearing loss. The Cochrane database of systematic reviews(1):Cd010151 https://doi.org/10.1002/14651858.CD010151.pub2.
[14] Xiong B, Liu Z, Liu Q, Peng Y, Wu H, Lin Y, et al. (2019) Missed hearing loss in tinnitus patients with normal audiograms. Hearing research.384:107826 https://doi.org/10.1016/j.heares.2019.107826.
[15] Parthasarathy S, Shetty HN. (2021) Manipulation of Hearing Aid Gain and Tinnitus Relief: A Paired Comparison Study. The journal of international advanced otology.17(2):145-9 https://doi.org/10.5152/jiao.2021.8873.
[16] Yoo HB, De Ridder D, Vanneste S. (2016) White Matter Changes in Tinnitus: Is It All Age and Hearing Loss? Brain connectivity.6(1):84-93 https://doi.org/10.1089/brain.2015.0380.
[17] Matamala MF, Nogales FF, Lardelli P, Navarro N. (1987) Metastatic granulosa cell tumor with pattern of sex cord tumor with annular tubules. International journal of gynecological pathology : official journal of the International Society of Gynecological Pathologists.6(2):185-93 https://doi.org/10.1097/00004347-198706000-00010.
[18] Clifford RE, Maihofer AX, Chatzinakos C, Coleman JRI, Daskalakis NP, Gasperi M, et al. (2024) Genetic architecture distinguishes tinnitus from hearing loss. Nature communications.15(1):614 https://doi.org/10.1038/s41467-024-44842-x.
[19] Williams W, Carter L. (2017) Tinnitus and leisure noise. International journal of audiology.56(4):219-25 https://doi.org/10.1080/14992027.2016.1250961.
[20] Martines F, Sireci F, Cannizzaro E, Costanzo R, Martines E, Mucia M, et al. (2015) Clinical observations and risk factors for tinnitus in a Sicilian cohort. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery.272(10):2719-29 https://doi.org/10.1007/s00405-014-3275-0.
[21] Veile A, Zimmermann H, Lorenz E, Becher H. (2018) Is smoking a risk factor for tinnitus? A systematic review, meta-analysis and estimation of the population attributable risk in Germany. BMJ open.8(2):e016589 https://doi.org/10.1136/bmjopen-2017-016589.
[22] Arnold ML, Dhar S, Lee DJ, Perreira KM, Pupo D, Tsalatsanis A, et al. (2022) Sex-Specific Prevalence, Demographic Characteristics, and Risk Factors of Tinnitus in the Hispanic Community Health Study/Study of Latinos. American journal of audiology.31(1):78-90 https://doi.org/10.1044/2021_aja-21-00138.
[23] Mazurek B, Boecking B, Brueggemann P. (2019) Association Between Stress and Tinnitus-New Aspects. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology.40(4):e467-e73 https://doi.org/10.1097/mao.0000000000002180.
[24] Musleh A, Alshehri S, Qobty A. (2022) Hyperlipidemia and its relation with tinnitus: Cross-sectional approach. Nigerian journal of clinical practice.25(7):1046-9 https://doi.org/10.4103/njcp.njcp_1465_21.
[25] Boecking B, Klasing S, Walter M, Brueggemann P, Nyamaa A, Rose M, et al. (2022) Vascular-Metabolic Risk Factors and Psychological Stress in Patients with Chronic Tinnitus. Nutrients.14(11) https://doi.org/10.3390/nu14112256.
[26] Lin X, Liu Y, Chen Z, Wei Y, Lin J, Chen C, et al. (2023) Association between depression and tinnitus in US adults: A nationally representative sample. Laryngoscope investigative otolaryngology.8(5):1365-75 https://doi.org/10.1002/lio2.1134.
[27] Mahboubi H, Oliaei S, Kiumehr S, Dwabe S, Djalilian HR. (2013) The prevalence and characteristics of tinnitus in the youth population of the United States. The Laryngoscope.123(8):2001-8 https://doi.org/10.1002/lary.24015.
[28] Lin FR, Thorpe R, Gordon-Salant S, Ferrucci L. (2011) Hearing loss prevalence and risk factors among older adults in the United States. The journals of gerontology Series A, Biological sciences and medical sciences.66(5):582-90 https://doi.org/10.1093/gerona/glr002.
[29] Seo JH, Kang JM, Hwang SH, Han KD, Joo YH. (2016) Relationship between tinnitus and suicidal behaviour in Korean men and women: a cross-sectional study. Clinical otolaryngology : official journal of ENT-UK ; official journal of Netherlands Society for Oto-Rhino-Laryngology & Cervico-Facial Surgery.41(3):222-7 https://doi.org/10.1111/coa.12500.
[30] Cheng YF, Xirasagar S, Kuo NW, Lin HC. (2023) Tinnitus and risk of attempted suicide: A one year follow-up study. Journal of affective disorders.322:141-5 https://doi.org/10.1016/j.jad.2022.11.009.
[31] Sanchez VA, Dinh PC, Jr., Rooker J, Monahan PO, Althouse SK, Fung C, et al. (2023) Prevalence and risk factors for ototoxicity after cisplatin-based chemotherapy. Journal of cancer survivorship : research and practice.17(1):27-39 https://doi.org/10.1007/s11764-022-01313-w.
[32] Feng X, Li W, Cheng M, Qiu W, Liang R, Li M, et al. (2022) Association of hearing loss with total and cause-specific mortality in US adults. Environmental science and pollution research international.29(4):5032-42 https://doi.org/10.1007/s11356-021-16038-z.
[33] Cao C, Cade WT, Li S, McMillan J, Friedenreich C, Yang L. (2021) Association of Balance Function With All-Cause and Cause-Specific Mortality Among US Adults. JAMA otolaryngology-- head & neck surgery.147(5):460-8 https://doi.org/10.1001/jamaoto.2021.0057.
[34] Martz E, Jelleberg C, Dougherty DD, Wolters C, Schneiderman A. (2018) Tinnitus, Depression, Anxiety, and Suicide in Recent Veterans: A Retrospective Analysis. Ear and hearing.39(6):1046-56 https://doi.org/10.1097/aud.0000000000000573.
[35] Leigh-Hunt N, Bagguley D, Bash K, Turner V, Turnbull S, Valtorta N, et al. (2017) An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public health.152:157-71 https://doi.org/10.1016/j.puhe.2017.07.035.
[36] Miaskowski C, Mastick J, Paul SM, Abrams G, Cheung S, Sabes JH, et al. (2018) Impact of chemotherapy-induced neurotoxicities on adult cancer survivors' symptom burden and quality of life. Journal of cancer survivorship : research and practice.12(2):234-45 https://doi.org/10.1007/s11764-017-0662-8.
[37] Khan A, Mubdi N, Budnick A, Feldman DR, Williams SW, Patel S, et al. (2020) The experience of hearing loss in adult survivors of childhood and young adult cancer: A qualitative study. Cancer.126(8):1776-83 https://doi.org/10.1002/cncr.32698.
[38] Hébert S, Lupien SJ. (2007) The sound of stress: blunted cortisol reactivity to psychosocial stress in tinnitus sufferers. Neuroscience letters.411(2):138-42 https://doi.org/10.1016/j.neulet.2006.10.028.
[39] Hébert S, Lupien SJ. (2009) Salivary cortisol levels, subjective stress, and tinnitus intensity in tinnitus sufferers during noise exposure in the laboratory. International journal of hygiene and environmental health.212(1):37-44 https://doi.org/10.1016/j.ijheh.2007.11.005.
[40] Hébert S, Paiement P, Lupien SJ. (2004) A physiological correlate for the intolerance to both internal and external sounds. Hearing research.190(1-2):1-9 https://doi.org/10.1016/s0378-5955(04)00021-8.
[41] Hasson D, Theorell T, Liljeholm-Johansson Y, Canlon B. (2009) Psychosocial and physiological correlates of self-reported hearing problems in male and female musicians in symphony orchestras. International journal of psychophysiology : official journal of the International Organization of Psychophysiology.74(2):93-100 https://doi.org/10.1016/j.ijpsycho.2009.07.009.
[42] Friberg E, Rosenhall U, Alexanderson K. (2014) Sickness absence and disability pension due to otoaudiological diagnoses: risk of premature death--a nationwide prospective cohort study. BMC public health.14:137 https://doi.org/10.1186/1471-2458-14-137.
[43] Li YL, Hsu YC, Lin CY, Wu JL. (2022) Sleep disturbance and psychological distress in adult patients with tinnitus. Journal of the Formosan Medical Association = Taiwan yi zhi.121(5):995-1002 https://doi.org/10.1016/j.jfma.2021.07.022.
[44] Pearson SE, Taylor J, Hoare DJ, Patel P, Baguley DM. (2019) Exploring the Experiences of Cancer Patients With Chemotherapy-Induced Ototoxicity: Qualitative Study Using Online Health Care Forums. JMIR cancer.5(1):e10883 https://doi.org/10.2196/10883.
[45] Karaaslan Ö, Kantekin Y, Hacımusalar Y, Dağıstan H. (2020) Anxiety sensitivities, anxiety and depression levels, and personality traits of patients with chronic subjective tinnitus: a case-control study. International journal of psychiatry in clinical practice.24(3):264-9 https://doi.org/10.1080/13651501.2020.1757117.
[46] Hamer M, Chida Y, Molloy GJ. (2009) Psychological distress and cancer mortality. Journal of psychosomatic research.66(3):255-8 https://doi.org/10.1016/j.jpsychores.2008.11.002.
[47] Knight KR, Kraemer DF, Neuwelt EA. (2005) Ototoxicity in children receiving platinum chemotherapy: underestimating a commonly occurring toxicity that may influence academic and social development. Journal of clinical oncology : official journal of the American Society of Clinical Oncology.23(34):8588-96 https://doi.org/10.1200/jco.2004.00.5355.
[48] Bisht M, Bist SS. (2011) Ototoxicity: the hidden menace. Indian journal of otolaryngology and head and neck surgery : official publication of the Association of Otolaryngologists of India.63(3):255-9 https://doi.org/10.1007/s12070-011-0151-8.
[49] Diaz KM, Shimbo D. (2013) Physical activity and the prevention of hypertension. Current hypertension reports.15(6):659-68 https://doi.org/10.1007/s11906-013-0386-8.
[50] Ekelund U, Tarp J, Steene-Johannessen J, Hansen BH, Jefferis B, Fagerland MW, et al. (2019) Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: systematic review and harmonised meta-analysis. BMJ (Clinical research ed).366:l4570 https://doi.org/10.1136/bmj.l4570.
[51] Wade KH, Carslake D, Sattar N, Davey Smith G, Timpson NJ. (2018) BMI and Mortality in UK Biobank: Revised Estimates Using Mendelian Randomization. Obesity (Silver Spring, Md).26(11):1796-806 https://doi.org/10.1002/oby.22313.
[52] Özbey-Yücel Ü, Uçar A, Aydoğan Z, Tokgoz-Yilmaz S, Beton S. (2023) The effects of dietary and physical activity interventions on tinnitus symptoms: An RCT. Auris, nasus, larynx.50(1):40-7 https://doi.org/10.1016/j.anl.2022.04.013.
[53] Biswas R, Lugo A, Genitsaridi E, Trpchevska N, Akeroyd MA, Cederroth CR, et al. (2021) Modifiable lifestyle-related risk factors for tinnitus in the general population: An overview of smoking, alcohol, body mass index and caffeine intake. Progress in brain research.263:1-24 https://doi.org/10.1016/bs.pbr.2021.04.005.
[54] Feldman RD, Gros R. (2010) Rapid vascular effects of steroids - a question of balance? The Canadian journal of cardiology.26 Suppl A:22a-6a https://doi.org/10.1016/s0828-282x(10)71057-6.
[55] Berkel C, Cacan E. (2021) Estrogen- and estrogen receptor (ER)-mediated cisplatin chemoresistance in cancer. Life sciences.286:120029 https://doi.org/10.1016/j.lfs.2021.120029.
[56] Rajoria S, Hanly E, Nicolini A, George AL, Geliebter J, Shin EJ, et al. (2014) Interlinking of hypoxia and estrogen in thyroid cancer progression. Current medicinal chemistry.21(11):1351-60 https://doi.org/10.2174/0929867321666131201142434.
[57] Bruce DG, Devine A, Prince RL. (2002) Recreational physical activity levels in healthy older women: the importance of fear of falling. Journal of the American Geriatrics Society.50(1):84-9 https://doi.org/10.1046/j.1532-5415.2002.50012.x.
[58] Jefferis BJ, Iliffe S, Kendrick D, Kerse N, Trost S, Lennon LT, et al. (2014) How are falls and fear of falling associated with objectively measured physical activity in a cohort of community-dwelling older men? BMC geriatrics.14:114 https://doi.org/10.1186/1471-2318-14-114.
[59] Yang L, Cao C, Kantor ED, Nguyen LH, Zheng X, Park Y, et al. (2019) Trends in Sedentary Behavior Among the US Population, 2001-2016. Jama.321(16):1587-97 https://doi.org/10.1001/jama.2019.3636.
[60] Agrawal Y, Carey JP, Della Santina CC, Schubert MC, Minor LB. (2009) Disorders of balance and vestibular function in US adults: data from the National Health and Nutrition Examination Survey, 2001-2004. Archives of internal medicine.169(10):938-44 https://doi.org/10.1001/archinternmed.2009.66.
[61] McCarthy E, Marchese VG, Shipper AG, Rock K, Felter C. (2024) Identifying causes of balance impairment and exploring sensory contributions to balance in pediatric oncology: A scoping review. Critical reviews in oncology/hematology.201:104425 https://doi.org/10.1016/j.critrevonc.2024.104425.
[62] Mulvaney J, Dabdoub A. (2012) Atoh1, an essential transcription factor in neurogenesis and intestinal and inner ear development: function, regulation, and context dependency. Journal of the Association for Research in Otolaryngology : JARO.13(3):281-93 https://doi.org/10.1007/s10162-012-0317-4.
[63] Pearson SE, Caimino C, Shabbir M, Baguley DM. (2022) The impact of chemotherapy-induced inner ear damage on quality of life in cancer survivors: a qualitative study. Journal of cancer survivorship : research and practice.16(5):976-87 https://doi.org/10.1007/s11764-021-01089-5.
 Figures
Figures References
References Peer
Peer Information
InformationFigure 1. Flowchart of this study.
Figure 2. Adjusted Hazard Ratios of all-cause and cause-specific mortality comparing tinnitus with no tinnitus, National Health and Nutrition Examination Survey, 1999-2004, 2011-2012, 2015-2016.
Figure 3. Stratified Hazard Ratios and 95% CIs for all-cause and cause-specific mortality according to tinnitus.
[1] Baguley D, McFerran D, Hall D. (2013) Tinnitus. Lancet (London, England).382(9904):1600-7 https://doi.org/10.1016/s0140-6736(13)60142-7.
[2] Langguth B, Kreuzer PM, Kleinjung T, De Ridder D. (2013) Tinnitus: causes and clinical management. The Lancet Neurology.12(9):920-30 https://doi.org/10.1016/s1474-4422(13)70160-1.
[3] Sharma A, Sood N, Munjal S, Panda N. (2021) Perception of Tinnitus Handicap And Stress Across Age Groups in Normal Hearing. The international tinnitus journal.25(1):13-7 https://doi.org/10.5935/0946-5448.2020004.
[4] Tunkel DE, Bauer CA, Sun GH, Rosenfeld RM, Chandrasekhar SS, Cunningham ER, Jr., et al. (2014) Clinical practice guideline: tinnitus. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery.151(2 Suppl):S1-s40 https://doi.org/10.1177/0194599814545325.
[5] Jafari Z, Kolb BE, Mohajerani MH. (2019) Age-related hearing loss and tinnitus, dementia risk, and auditory amplification outcomes. Ageing research reviews.56:100963 https://doi.org/10.1016/j.arr.2019.100963.
[6] Friberg E, Jansson C, Mittendorfer-Rutz E, Rosenhall U, Alexanderson K. (2012) Sickness absence due to otoaudiological diagnoses and risk of disability pension: a nationwide Swedish prospective cohort study. PloS one.7(1):e29966 https://doi.org/10.1371/journal.pone.0029966.
[7] Esmaili AA, Renton J. (2018) A review of tinnitus. Australian journal of general practice.47(4):205-8 https://doi.org/10.31128/ajgp-12-17-4420.
[8] Choi J, Lee CH, Kim SY. (2021) Association of Tinnitus with Depression in a Normal Hearing Population. Medicina (Kaunas, Lithuania).57(2) https://doi.org/10.3390/medicina57020114.
[9] Granjeiro RC, Kehrle HM, de Oliveira TS, Sampaio AL, de Oliveira CA. (2013) Is the degree of discomfort caused by tinnitus in normal-hearing individuals correlated with psychiatric disorders? Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery.148(4):658-63 https://doi.org/10.1177/0194599812473554.
[10] Huang YS, Koo M, Chen JC, Hwang JH. (2017) The association between tinnitus and the risk of ischemic cerebrovascular disease in young and middle-aged patients: A secondary case-control analysis of a nationwide, population-based health claims database. PloS one.12(11):e0187474 https://doi.org/10.1371/journal.pone.0187474.
[11] Chu HT, Liang CS, Yeh TC, Hu LY, Yang AC, Tsai SJ, et al. (2020) Tinnitus and risk of Alzheimer's and Parkinson's disease: a retrospective nationwide population-based cohort study. Scientific reports.10(1):12134 https://doi.org/10.1038/s41598-020-69243-0.
[12] Loiselle AR, Neustaeter A, de Kleine E, van Dijk P, Jansonius NM. (2020) Associations between tinnitus and glaucoma suggest a common mechanism: A clinical and population-based study. Hearing research.386:107862 https://doi.org/10.1016/j.heares.2019.107862.
[13] Hoare DJ, Edmondson-Jones M, Sereda M, Akeroyd MA, Hall D. (2014) Amplification with hearing aids for patients with tinnitus and co-existing hearing loss. The Cochrane database of systematic reviews(1):Cd010151 https://doi.org/10.1002/14651858.CD010151.pub2.
[14] Xiong B, Liu Z, Liu Q, Peng Y, Wu H, Lin Y, et al. (2019) Missed hearing loss in tinnitus patients with normal audiograms. Hearing research.384:107826 https://doi.org/10.1016/j.heares.2019.107826.
[15] Parthasarathy S, Shetty HN. (2021) Manipulation of Hearing Aid Gain and Tinnitus Relief: A Paired Comparison Study. The journal of international advanced otology.17(2):145-9 https://doi.org/10.5152/jiao.2021.8873.
[16] Yoo HB, De Ridder D, Vanneste S. (2016) White Matter Changes in Tinnitus: Is It All Age and Hearing Loss? Brain connectivity.6(1):84-93 https://doi.org/10.1089/brain.2015.0380.
[17] Matamala MF, Nogales FF, Lardelli P, Navarro N. (1987) Metastatic granulosa cell tumor with pattern of sex cord tumor with annular tubules. International journal of gynecological pathology : official journal of the International Society of Gynecological Pathologists.6(2):185-93 https://doi.org/10.1097/00004347-198706000-00010.
[18] Clifford RE, Maihofer AX, Chatzinakos C, Coleman JRI, Daskalakis NP, Gasperi M, et al. (2024) Genetic architecture distinguishes tinnitus from hearing loss. Nature communications.15(1):614 https://doi.org/10.1038/s41467-024-44842-x.
[19] Williams W, Carter L. (2017) Tinnitus and leisure noise. International journal of audiology.56(4):219-25 https://doi.org/10.1080/14992027.2016.1250961.
[20] Martines F, Sireci F, Cannizzaro E, Costanzo R, Martines E, Mucia M, et al. (2015) Clinical observations and risk factors for tinnitus in a Sicilian cohort. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery.272(10):2719-29 https://doi.org/10.1007/s00405-014-3275-0.
[21] Veile A, Zimmermann H, Lorenz E, Becher H. (2018) Is smoking a risk factor for tinnitus? A systematic review, meta-analysis and estimation of the population attributable risk in Germany. BMJ open.8(2):e016589 https://doi.org/10.1136/bmjopen-2017-016589.
[22] Arnold ML, Dhar S, Lee DJ, Perreira KM, Pupo D, Tsalatsanis A, et al. (2022) Sex-Specific Prevalence, Demographic Characteristics, and Risk Factors of Tinnitus in the Hispanic Community Health Study/Study of Latinos. American journal of audiology.31(1):78-90 https://doi.org/10.1044/2021_aja-21-00138.
[23] Mazurek B, Boecking B, Brueggemann P. (2019) Association Between Stress and Tinnitus-New Aspects. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology.40(4):e467-e73 https://doi.org/10.1097/mao.0000000000002180.
[24] Musleh A, Alshehri S, Qobty A. (2022) Hyperlipidemia and its relation with tinnitus: Cross-sectional approach. Nigerian journal of clinical practice.25(7):1046-9 https://doi.org/10.4103/njcp.njcp_1465_21.
[25] Boecking B, Klasing S, Walter M, Brueggemann P, Nyamaa A, Rose M, et al. (2022) Vascular-Metabolic Risk Factors and Psychological Stress in Patients with Chronic Tinnitus. Nutrients.14(11) https://doi.org/10.3390/nu14112256.
[26] Lin X, Liu Y, Chen Z, Wei Y, Lin J, Chen C, et al. (2023) Association between depression and tinnitus in US adults: A nationally representative sample. Laryngoscope investigative otolaryngology.8(5):1365-75 https://doi.org/10.1002/lio2.1134.
[27] Mahboubi H, Oliaei S, Kiumehr S, Dwabe S, Djalilian HR. (2013) The prevalence and characteristics of tinnitus in the youth population of the United States. The Laryngoscope.123(8):2001-8 https://doi.org/10.1002/lary.24015.
[28] Lin FR, Thorpe R, Gordon-Salant S, Ferrucci L. (2011) Hearing loss prevalence and risk factors among older adults in the United States. The journals of gerontology Series A, Biological sciences and medical sciences.66(5):582-90 https://doi.org/10.1093/gerona/glr002.
[29] Seo JH, Kang JM, Hwang SH, Han KD, Joo YH. (2016) Relationship between tinnitus and suicidal behaviour in Korean men and women: a cross-sectional study. Clinical otolaryngology : official journal of ENT-UK ; official journal of Netherlands Society for Oto-Rhino-Laryngology & Cervico-Facial Surgery.41(3):222-7 https://doi.org/10.1111/coa.12500.
[30] Cheng YF, Xirasagar S, Kuo NW, Lin HC. (2023) Tinnitus and risk of attempted suicide: A one year follow-up study. Journal of affective disorders.322:141-5 https://doi.org/10.1016/j.jad.2022.11.009.
[31] Sanchez VA, Dinh PC, Jr., Rooker J, Monahan PO, Althouse SK, Fung C, et al. (2023) Prevalence and risk factors for ototoxicity after cisplatin-based chemotherapy. Journal of cancer survivorship : research and practice.17(1):27-39 https://doi.org/10.1007/s11764-022-01313-w.
[32] Feng X, Li W, Cheng M, Qiu W, Liang R, Li M, et al. (2022) Association of hearing loss with total and cause-specific mortality in US adults. Environmental science and pollution research international.29(4):5032-42 https://doi.org/10.1007/s11356-021-16038-z.
[33] Cao C, Cade WT, Li S, McMillan J, Friedenreich C, Yang L. (2021) Association of Balance Function With All-Cause and Cause-Specific Mortality Among US Adults. JAMA otolaryngology-- head & neck surgery.147(5):460-8 https://doi.org/10.1001/jamaoto.2021.0057.
[34] Martz E, Jelleberg C, Dougherty DD, Wolters C, Schneiderman A. (2018) Tinnitus, Depression, Anxiety, and Suicide in Recent Veterans: A Retrospective Analysis. Ear and hearing.39(6):1046-56 https://doi.org/10.1097/aud.0000000000000573.
[35] Leigh-Hunt N, Bagguley D, Bash K, Turner V, Turnbull S, Valtorta N, et al. (2017) An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public health.152:157-71 https://doi.org/10.1016/j.puhe.2017.07.035.
[36] Miaskowski C, Mastick J, Paul SM, Abrams G, Cheung S, Sabes JH, et al. (2018) Impact of chemotherapy-induced neurotoxicities on adult cancer survivors' symptom burden and quality of life. Journal of cancer survivorship : research and practice.12(2):234-45 https://doi.org/10.1007/s11764-017-0662-8.
[37] Khan A, Mubdi N, Budnick A, Feldman DR, Williams SW, Patel S, et al. (2020) The experience of hearing loss in adult survivors of childhood and young adult cancer: A qualitative study. Cancer.126(8):1776-83 https://doi.org/10.1002/cncr.32698.
[38] Hébert S, Lupien SJ. (2007) The sound of stress: blunted cortisol reactivity to psychosocial stress in tinnitus sufferers. Neuroscience letters.411(2):138-42 https://doi.org/10.1016/j.neulet.2006.10.028.
[39] Hébert S, Lupien SJ. (2009) Salivary cortisol levels, subjective stress, and tinnitus intensity in tinnitus sufferers during noise exposure in the laboratory. International journal of hygiene and environmental health.212(1):37-44 https://doi.org/10.1016/j.ijheh.2007.11.005.
[40] Hébert S, Paiement P, Lupien SJ. (2004) A physiological correlate for the intolerance to both internal and external sounds. Hearing research.190(1-2):1-9 https://doi.org/10.1016/s0378-5955(04)00021-8.
[41] Hasson D, Theorell T, Liljeholm-Johansson Y, Canlon B. (2009) Psychosocial and physiological correlates of self-reported hearing problems in male and female musicians in symphony orchestras. International journal of psychophysiology : official journal of the International Organization of Psychophysiology.74(2):93-100 https://doi.org/10.1016/j.ijpsycho.2009.07.009.
[42] Friberg E, Rosenhall U, Alexanderson K. (2014) Sickness absence and disability pension due to otoaudiological diagnoses: risk of premature death--a nationwide prospective cohort study. BMC public health.14:137 https://doi.org/10.1186/1471-2458-14-137.
[43] Li YL, Hsu YC, Lin CY, Wu JL. (2022) Sleep disturbance and psychological distress in adult patients with tinnitus. Journal of the Formosan Medical Association = Taiwan yi zhi.121(5):995-1002 https://doi.org/10.1016/j.jfma.2021.07.022.
[44] Pearson SE, Taylor J, Hoare DJ, Patel P, Baguley DM. (2019) Exploring the Experiences of Cancer Patients With Chemotherapy-Induced Ototoxicity: Qualitative Study Using Online Health Care Forums. JMIR cancer.5(1):e10883 https://doi.org/10.2196/10883.
[45] Karaaslan Ö, Kantekin Y, Hacımusalar Y, Dağıstan H. (2020) Anxiety sensitivities, anxiety and depression levels, and personality traits of patients with chronic subjective tinnitus: a case-control study. International journal of psychiatry in clinical practice.24(3):264-9 https://doi.org/10.1080/13651501.2020.1757117.
[46] Hamer M, Chida Y, Molloy GJ. (2009) Psychological distress and cancer mortality. Journal of psychosomatic research.66(3):255-8 https://doi.org/10.1016/j.jpsychores.2008.11.002.
[47] Knight KR, Kraemer DF, Neuwelt EA. (2005) Ototoxicity in children receiving platinum chemotherapy: underestimating a commonly occurring toxicity that may influence academic and social development. Journal of clinical oncology : official journal of the American Society of Clinical Oncology.23(34):8588-96 https://doi.org/10.1200/jco.2004.00.5355.
[48] Bisht M, Bist SS. (2011) Ototoxicity: the hidden menace. Indian journal of otolaryngology and head and neck surgery : official publication of the Association of Otolaryngologists of India.63(3):255-9 https://doi.org/10.1007/s12070-011-0151-8.
[49] Diaz KM, Shimbo D. (2013) Physical activity and the prevention of hypertension. Current hypertension reports.15(6):659-68 https://doi.org/10.1007/s11906-013-0386-8.
[50] Ekelund U, Tarp J, Steene-Johannessen J, Hansen BH, Jefferis B, Fagerland MW, et al. (2019) Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: systematic review and harmonised meta-analysis. BMJ (Clinical research ed).366:l4570 https://doi.org/10.1136/bmj.l4570.
[51] Wade KH, Carslake D, Sattar N, Davey Smith G, Timpson NJ. (2018) BMI and Mortality in UK Biobank: Revised Estimates Using Mendelian Randomization. Obesity (Silver Spring, Md).26(11):1796-806 https://doi.org/10.1002/oby.22313.
[52] Özbey-Yücel Ü, Uçar A, Aydoğan Z, Tokgoz-Yilmaz S, Beton S. (2023) The effects of dietary and physical activity interventions on tinnitus symptoms: An RCT. Auris, nasus, larynx.50(1):40-7 https://doi.org/10.1016/j.anl.2022.04.013.
[53] Biswas R, Lugo A, Genitsaridi E, Trpchevska N, Akeroyd MA, Cederroth CR, et al. (2021) Modifiable lifestyle-related risk factors for tinnitus in the general population: An overview of smoking, alcohol, body mass index and caffeine intake. Progress in brain research.263:1-24 https://doi.org/10.1016/bs.pbr.2021.04.005.
[54] Feldman RD, Gros R. (2010) Rapid vascular effects of steroids - a question of balance? The Canadian journal of cardiology.26 Suppl A:22a-6a https://doi.org/10.1016/s0828-282x(10)71057-6.
[55] Berkel C, Cacan E. (2021) Estrogen- and estrogen receptor (ER)-mediated cisplatin chemoresistance in cancer. Life sciences.286:120029 https://doi.org/10.1016/j.lfs.2021.120029.
[56] Rajoria S, Hanly E, Nicolini A, George AL, Geliebter J, Shin EJ, et al. (2014) Interlinking of hypoxia and estrogen in thyroid cancer progression. Current medicinal chemistry.21(11):1351-60 https://doi.org/10.2174/0929867321666131201142434.
[57] Bruce DG, Devine A, Prince RL. (2002) Recreational physical activity levels in healthy older women: the importance of fear of falling. Journal of the American Geriatrics Society.50(1):84-9 https://doi.org/10.1046/j.1532-5415.2002.50012.x.
[58] Jefferis BJ, Iliffe S, Kendrick D, Kerse N, Trost S, Lennon LT, et al. (2014) How are falls and fear of falling associated with objectively measured physical activity in a cohort of community-dwelling older men? BMC geriatrics.14:114 https://doi.org/10.1186/1471-2318-14-114.
[59] Yang L, Cao C, Kantor ED, Nguyen LH, Zheng X, Park Y, et al. (2019) Trends in Sedentary Behavior Among the US Population, 2001-2016. Jama.321(16):1587-97 https://doi.org/10.1001/jama.2019.3636.
[60] Agrawal Y, Carey JP, Della Santina CC, Schubert MC, Minor LB. (2009) Disorders of balance and vestibular function in US adults: data from the National Health and Nutrition Examination Survey, 2001-2004. Archives of internal medicine.169(10):938-44 https://doi.org/10.1001/archinternmed.2009.66.
[61] McCarthy E, Marchese VG, Shipper AG, Rock K, Felter C. (2024) Identifying causes of balance impairment and exploring sensory contributions to balance in pediatric oncology: A scoping review. Critical reviews in oncology/hematology.201:104425 https://doi.org/10.1016/j.critrevonc.2024.104425.
[62] Mulvaney J, Dabdoub A. (2012) Atoh1, an essential transcription factor in neurogenesis and intestinal and inner ear development: function, regulation, and context dependency. Journal of the Association for Research in Otolaryngology : JARO.13(3):281-93 https://doi.org/10.1007/s10162-012-0317-4.
[63] Pearson SE, Caimino C, Shabbir M, Baguley DM. (2022) The impact of chemotherapy-induced inner ear damage on quality of life in cancer survivors: a qualitative study. Journal of cancer survivorship : research and practice.16(5):976-87 https://doi.org/10.1007/s11764-021-01089-5.
Peer-review Terminology
Identity transparency: Single anonymized
Reviewer interacts with: Editor
Details
This is an open access article under the terms of the Creative Commons Attribution License(http://creativecommons.org/licenses/by/4.0/), which permits use, distribution and reproduction in any medium, provided the original work is properly cited.
Publication History
Received 2025-04-02
Accepted 2025-05-10
Published 2025-05-15