


Abstract
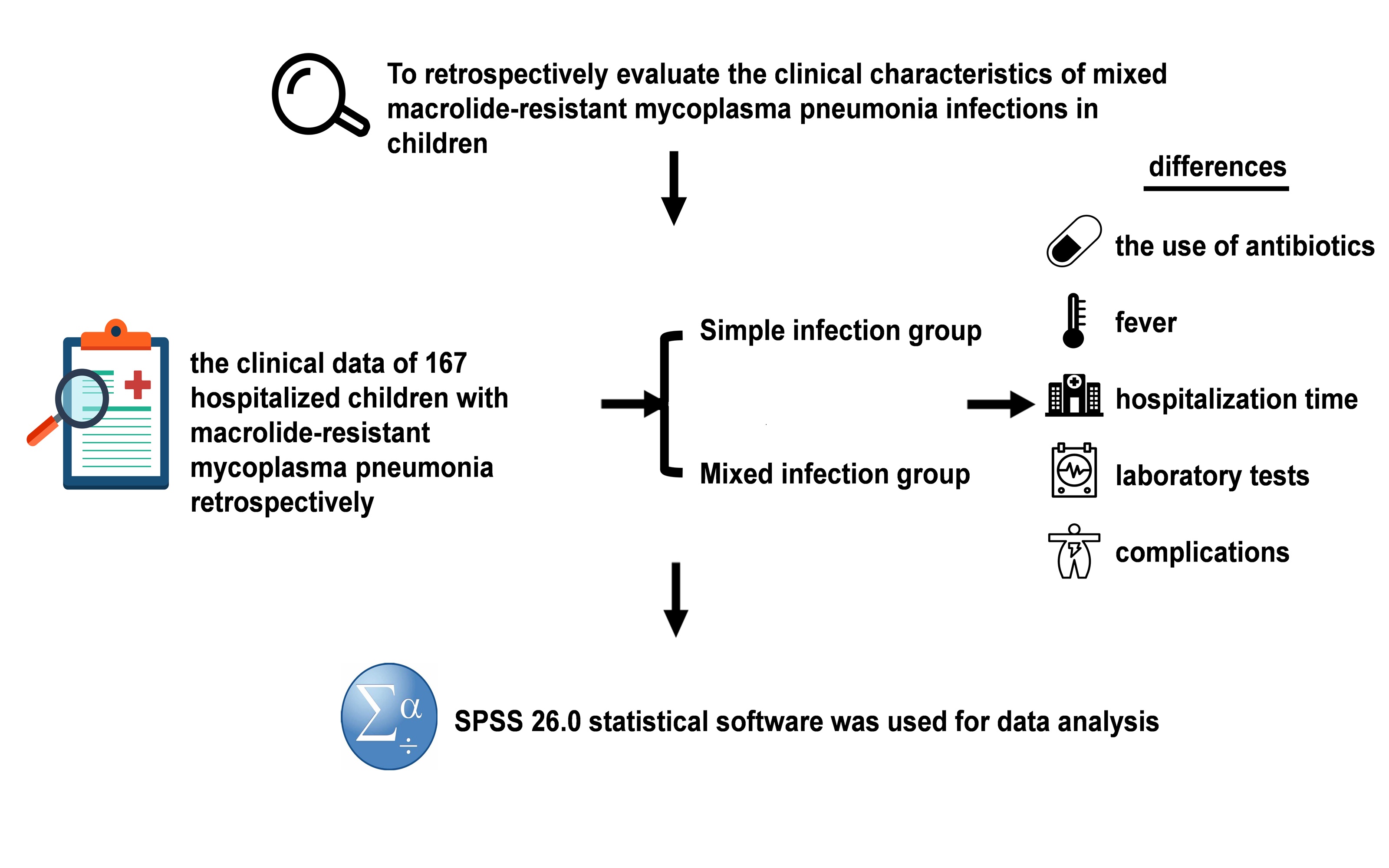
Purpose:Epidemiological data from Asia have documented the rapid and widespread emergence of macrolide resistance in Mycoplasma pneumoniae (MP). This paper aims to retrospectively evaluate the clinical characteristics of mixed macrolide-resistant Mycoplasma pneumoniae (MRMP) infections in children.
Methods:The study included 167 hospitalized children with MRMP. We analyzed the children's clinical data retrospectively, and compared the differences in the use of antibiotics, fever, hospitalization time, laboratory tests and complications between the mixed infection group and the separately infected group before admission.
Results:Compared with the separately infected group, hospitalized children with mixed infection had a longer hospital stay, and there was a significant difference between the two (P < 0.05); Alanine aminotransferase (ALT), aspartate aminotransferase (AST), lactate dehydrogenase (LDH), creatine kinase (CK), and platelet count (PLT) of children in the mixed infection group were significantly higher than those in the separately infected group (P < 0.05); and the incidence of hepatic function impairment, cardiac enzyme profile abnormality, and pleural effusion in the children in the mixed infection group was higher than that in the separately infected group (P < 0.01).
Conclusion:Patients with MRMP combined with mixed infections had prolonged hospital stays, increased systemic inflammatory response, and increased incidence of extrapulmonary complications compared with those with simple infections.
Keywords:Mycoplasma pneumoniae; Macrolide resistance; Mixed infection; Hospitalized children
Introduction
MP is one of the major pathogens causing community-acquired pneumonia (CAP) in children and adolescents, accounting for up to about 40% of cases[1] . While pneumonia caused by MP is typically a self-limiting disease[2] , some patients may develop refractory Mycoplasma pneumoniae pneumonia (RMPP)[3] or extrapulmonary complications[4,5] . Macrolides are currently the first-line agents for treating Mycoplasma pneumoniae pneumonia (MPP) in pediatric populations. However, the widespread use of macrolides has resulted in a sustained increase in antibiotic resistance prevalence, with significant regional variations. Mutations at nucleotide sites A2063, A2064, A2067, and C2617 within the 23S rRNA domain V of MP are recognized as markers of MRMP[5] . Among these, the A2063G mutation is the most frequently identified in resistant isolates[7] . Mixed infections have been reported to be more common in children with MPP, in which disease severity is higher than in single pathogen infections[8,9] . Relevant studies have shown that co-infection of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) with MP during the Coronavirus Disease 2019 (COVID-19) pandemic may lead to prolonged Intensive Care Unit (ICU) hospitalization or exacerbation of clinical symptoms in patients[10,11] .
In this study, we analyzed the clinical characteristics and laboratory test results of children with MRMP and mixed infections in Hefei, aiming to identify children with MRMP with mixed infections at an early stage, and to guide clinicians to intervene in the rational use of antibiotics and therapeutic measures as a means of reducing complications, shortening the hospitalization time of the children, and improving the prognosis.
Methods
Study Design and Population
The clinical data of 167 children diagnosed with MPP in the First Affiliated Hospital of Anhui Medical University were collected. All children were diagnosed with MPP according to WHO's CAP clinical diagnostic criteria[12] , including symptoms and chest X-rays assessed by clinicians. Inclusion criteria: (1) age from 5 months to 15 years; (2) positive MP PCR or positive serologic tests; (3) macrolide antibiotic resistance; (4) complete clinical data. Exclusion criteria: (1) immunocompromised; (2) chronic lung disease (except asthma), chronic heart disease; (3) diseases of the blood system; (4) incomplete clinical data.
Data Collection and Variables
The clinical data of the children were collected, including gender, age, previous antibiotic use during the disease and clinical symptoms such as fever, cough, sputum, rash, and duration of symptoms before hospitalization. In addition white blood cell count (WBC), percentage of neutrophils (NEU), percentage of monocytes (MON), PLT, fibrinogen (FIB), prothrombin time (TT), D-dimer (DD), fibrinogen degradation product (FDP), CK, urea (UREA), blood creatinine (CRE ), blood uric acid (UA), glomerular filtration rate (eGFR), C-reactive protein (CRP), procalcitoninogen (PCT), activated partial thromboplastin time (APTT), prothrombin time (PT), ALT, AST, LDH, and total protein (TP), chest X-ray, and complications: Hepatic impairment, pleural effusion, ketonuria, pulmonary atelectasis, coagulation disorders, micronutrient deficiencies and abnormalities in cardiac enzyme profiles.
Detection of MP drug resistance genes
The presence of mutations at the A2063 and A2064 loci was determined by pyrophosphate sequencing of the two portions of the 23S rRNA gene structural domain V. The extracted nucleic acids were reverse transcribed into the nucleic acids of the A2063 and A2064 loci. The extracted nucleic acids were reverse transcribed into cDNA for amplification (11121ES, Yeason Biotech Co., Shanghai, China). Positions 2063 and 2064 in the structural domain of the 23SrRNA gene were amplified using PCR as described below. PCR system: ddH20 16 μl, 2×Taq Master Mix 25 μl, Forward primer1 (10 μM) 2 μl, Reverse primer2 (10 μM) 2 μl. cDNA 5μl, the total system was 50μl. program: 95°C 3min; 95°C 15S, 60°C 15S, 72°C 60S cycle 35 times; 72°C 5min. the PCR products were compared with the MP standard gene (23SrRNA gene, GenBank no. X 68422) after bidirectional sequencing by Anhui General Biological Company[13] .
Statistical analysis
SPSS 26.0 statistical software was used for data analysis. According to data types, categorical variables were expressed as frequencies and percentages, and continuous variables were expressed as medians and quartiles. Normal distribution was expressed as mean ± standard deviation, and non-normal distribution was expressed as interquartile spacing. When comparisons were made between two groups, normal distribution was tested by the t test; non-normal tests were tested by the rank sum test. Count data were compared using χ2 or corrected χ2. p<0.05 was considered statistically significant.
Ethics Approval
The current investigation was duly approved by the human ethics council of Anhui Medical University's First Affiliated Hospital (Approval No: Quick-PJ 2023-08-41). The written informed consent was obtained from patients in accordance with the Declaration of Helsinki.
Results
Study of drug-resistant gene mutations of MP
In this study, 167 MP nucleic acid positive patients were amplified and sequenced at the above loci. The results showed that the A2063G mutation in the V region of the 23SrRNA gene was found in all 167 (167/167,100%) patients, and no drug-resistant mutation was found in the A2064G/A2064C locus.
Comparison of clinical symptoms on admission between the two groups
According to the results in Table 1, most of the patients were on antibiotics before admission. The length of hospitalization in the mixed infection group was significantly longer than that in the simple infection group, and the difference between the two groups was statistically significant (Z=-6.607, p < 0.001); however, the clinical symptoms exhibited by the patients, such as fever, cough, sputum, vomiting, rash, and dizziness, were not statistically significant between the two groups.
Table 1 Comparison between clinical symptoms in simple and mixed infection groups
|
Simple infection group (n=117) |
Mixed infection group (n=50) |
c2/t/Z value |
p value |
|
|
Use of antibiotics before admission |
116(99.1) |
49(98.0) |
0.000# |
>0.999 |
|
Length of hospitalization (d) |
4.0(4.0,6.0) |
7.0(5.8,8.0) |
-6.607 |
<0.001 |
|
ICU |
14(11.9) |
10(20.0) |
1.837 |
0.175 |
|
Fever |
114(97.4 ) |
48(96.0) |
0.249 |
0.618 |
|
Cough |
114(97.4) |
47(94.0) |
1.194 |
0.275 |
|
phlegm |
72(61.5) |
24(48.0) |
2.627 |
0.105 |
|
Vomiting |
14(28.0) |
10(20.0) |
1.837 |
0.175 |
|
Rash |
4(3.4) |
0(0) |
0.594# |
0.441 |
|
Dizziness |
2(1.7) |
0(0) |
0.024# |
0.878 |
# chi-square test continuity correction
Comparison of relevant laboratory test indexes between the two groups
The PLT, ALT, AST, LDH and CK of the children in the mixed infection group were elevated and higher than those in the simple infection group, and the difference was statistically significant (P < 0.05), especially for ALT and LDH (P < 0.001). While other blood routine related indexes, coagulation function indexes and renal function indexes were compared, the difference was not statistically significant (P > 0.05). See Table 2.
Table 2 Comparison of laboratory test results between simple infection group and mixed infection group
|
Simple infection group |
Mixed infection group |
t/Z value |
P value |
|
|
WBC |
6.66(5.61,8.89) |
7.12(5.82,9.23) |
-1.213 |
0.225 |
|
NEU |
59.98±12.46 |
61.04±13.70 |
-0.490 |
0.624 |
|
LYM |
31.00±12.05 |
30.68±13.34 |
0.150 |
0.881 |
|
MON |
6.50(5.35,8.30) |
5.95(4.78,7.75) |
-1.384 |
0.166 |
|
PLT |
301.00(251.00,362.50) |
344.00(266.00,414.25) |
-1.966 |
0.049 |
|
CRP |
9.24(3.11,20.56) |
10.33(2.21,20.21) |
-0.687 |
0.492 |
|
PCT |
0.08(0.05,0.10) |
0.08(0.05,0.14) |
-0.055 |
0.956 |
|
PT |
12.60(12.10,13.00) |
12.58(12.10,13.00) |
-0.005 |
0.996 |
|
APTT |
38.78±5.76 |
38.91±4.73 |
-0.160 |
0.873 |
|
FIB |
4.59(4.06,5.04) |
4.50(3.94,5.03) |
-0.650 |
0.516 |
|
TT |
16.80(16.20,17.20) |
16.57(16.05,17.20) |
-1.269 |
0.204 |
|
DD |
0.68(0.42,1.06) |
0.55(0.36,0.89) |
-1.595 |
0.111 |
|
FDP |
2.71(2.05,3.86) |
2.33(1.52,3.69) |
-1.319 |
0.187 |
|
TP |
68.4(64.9,72.7) |
67.4(64.1,72.18) |
-0.606 |
0.544 |
|
ALT |
16.00(13.00,20.00) |
23.00(15.00,33.25) |
-4.073 |
<0.001 |
|
AST |
29.00(24.50,34.00) |
31.50(25.00,49.25) |
-2.223 |
0.026 |
|
LDH |
289.00(259.00,346.00) |
342.50(304.25,450.25) |
-4.108 |
<0.001 |
|
CK |
71.00(45.5,106.00) |
92.00(60.25,230.20) |
-2.473 |
0.013 |
|
UREA |
3.19(2.47,3.83) |
3.23(2.64,3.89) |
-1.148 |
0.251 |
|
CRE |
32.60±7.79 |
31.03±7.61 |
1.198 |
0.860 |
|
UA |
221.00(185.50,289.00) |
214.5(185.00,260.00) ) |
-0.620 |
0.535 |
|
eGFR |
185.00(178.00,209.00) |
195.00(179.25,223.50) |
-0.699 |
0.485 |
Comparison of complications between the two groups
The incidence of complications of pleural effusion, liver function impairment and cardiac enzyme spectrum abnormality was higher in the mixed infection group than in the simple infection group, and the difference was statistically significant (P < 0.05). There was no significant difference in the incidence of coagulation dysfunction, ketonuria, pulmonary atelectasis and micronutrient deficiency between the two groups (P > 0.05).
Table 3 Comparison of complications between the simple infection group and the mixed infection group (cases (x/%))
Table 3 Comparison of complications between the simple infection group and the mixed infection group (cases (x/%))
|
Simple infection group |
Mixed infection group |
c2/t/Z value |
P value |
|
|
Pleural effusion |
5(4.3) |
13(26.0) |
17.195 |
<0.001 |
|
Lung atelectasis |
17(14.5) |
9(18.0) |
0.321 |
0.571 |
|
Hepatic impairment |
5(4.3) |
10(20.0) |
10.597 |
0.001 |
|
Ketonuria |
7(6.0) |
7(14.0) |
1.981 |
0.159 |
|
Coagulation abnormalities |
36(30.8) |
10(20.0) |
2.124 |
0.145 |
|
Abnormal cardiac enzyme profile |
1(0.8) |
7(14.0) |
13.727 |
<0.001 |
|
Micronutrient deficiencies |
44(37.6) |
17(34.0) |
0.197 |
0.658 |
Discussion
MP is microorganisms intermediate between cells and viruses that cause respiratory infections[14] and is one of the major pathogens causing community-acquired pneumonia in children, prevalent in children aged 4-6 years[15] .MP infections exhibit a range of signs and symptoms from asymptomatic infections to severe and potentially fatal intra- and extra-pulmonary complications.
It has been documented that the co-infection rate of MP with other respiratory infection pathogens is 88.49%[16] . However, in some cases, these co-infections can lead to severe disease. In this study, when MRMP was co-infected with other pathogens, the length of hospitalization was prolonged, and in addition, the serum levels of ALT, AST, LDH, and CK were increased in patients, which may be related to the extrapulmonary complications of MP infection and the activation of the immune response in children's organisms[17] .
In recent years for the treatment of MPP in children the first choice is macrolides, which to some extent can relieve the symptoms of patients. However, overuse of macrolides has resulted in the development of macrolide-resistant antibiotic resistance. Since the first isolation of drug-resistant strains from patients in Japan in 2001, countries have begun to emphasize and monitor the occurrence of resistance rates. In China, there is some variability in the resistance rate in each region. For example, the resistance rate was 60.33% in Guangyuan[18] and 93.88% in Yunnan[19] . The results of this study found that the resistance mutation rate in Hefei region during the MP epidemic was as high as 100% and was a mutation at the A2063G locus, which is the mutation locus with the highest incidence in China at present[20] .
Research has found that during follow-up of some pediatric patients treated with azithromycin according to standard protocols, some patients developed antibiotic-resistant gene mutations within 2 to 4 weeks[18] , indicating that antibiotics can induce resistant mutations or select for resistant strains in the short term. This highlights the importance of avoiding unnecessary antibiotic use. Additionally, studies have shown that macrolide antibiotics have some efficacy against MRMP infections, but this is not because MRMP is sensitive to macrolide antibiotics, but rather due to the self-limiting nature of MP infections and the anti-inflammatory effects of macrolide drugs[21] . Other studies have also found that the use of macrolide antibiotics does not provide significant benefits for mild MP infections[22] . Therefore, the standardized use of macrolide drugs is essential. It is crucial to continue strictly adhering to the standards for the use of macrolide antibiotics to reduce the emergence and spread of drug-resistant strains. Clinicians should promptly monitor the drug resistance of MRMP patients and rationally select antimicrobial drugs to minimize the emergence of drug-resistant strains, thereby providing a scientific basis for MP treatment. Avoiding unnecessary antibiotic use and curbing the emergence of microbial drug resistance is of critical importance to children, families, and the healthcare system.
Children with MPP primarily present with fever and cough. Early pulmonary signs may not be prominent, but as the condition progresses, decreased breath sounds, dry rales, and wet rales may appear. Severe Mycoplasma pneumoniae pneumonia (SMPP) typically occurs around one week into the illness, often accompanied by pulmonary and extrapulmonary complications. A small number of MPP cases may progress to critical illness, often presenting with prominent symptoms of dyspnea and respiratory failure. The Guidelines for the Diagnosis and Treatment of Mycoplasma Pneumonia in Children (2023 Edition) emphasize that the key to managing mycoplasma pneumonia lies in the early identification and treatment of SMPP and fulminant Mycoplasma pneumoniae pneumonia (FMPP). The optimal treatment window is within 5–10 days after the onset of fever. Early diagnosis and intervention for children with MP are crucial in preventing the occurrence of complications.
This study indicates that the incidence of liver function impairment and complications is higher in the mixed infection group than in the single infection group. Previous studies have shown that there are differences in LDH elevation between the resistant group and the sensitive group, while CRP changes are similar[23] . This not only confirms that MRMP exhibits a stronger immune response but also suggests that LDH is a more sensitive immunological indicator than CRP. Imaging findings are one of the primary bases for clinically assessing the severity of MPP in children and evaluating prognosis. Early imaging examinations aid in the early identification and treatment of SMPP and FMPP, enabling the development of individualized treatment plans based on classification. For mild cases, systemic corticosteroids should not be routinely used in addition to anti-MP therapy. However, corticosteroids are frequently used in cases of MP infection complicated by excessive inflammatory responses. Studies have shown that corticosteroids can rapidly improve clinical and imaging findings in severe MPP[24] . The Chinese Expert Consensus on the Diagnosis and Treatment of MPP in Children also states that systemic corticosteroids may be considered for acute-onset, rapidly progressing, and severe MPP[25] .
Domestic studies have found that among MP-associated viral infections, respiratory syncytial virus accounts for the highest proportion, While among MP-associated bacterial infections, Streptococcus pneumoniae and Klebsiella pneumoniae are more common[26] . Children with Epstein-Barr virus(EBV)-associated MP infections experience longer fever durations and are more prone to respiratory distress or pleural effusion, suggesting that during clinical treatment, when prolonged fever, respiratory distress, or pleural effusion occurs, the possibility of co-infection should be considered[27] . In the Taipei study, 64.7% of patients requiring ICU admission presented with pleural effusion, indicating a high incidence of pleural effusion as a comorbidity[28] , which is similar to our results. WBC, PLT, Hb levels, fever duration, dyspnea, and pleural effusion are useful in diagnosing MPP in children with EBV infection. Multi-organ damage is exacerbated by mixed infections, which may involve complex immune response mechanisms. Some scholars have suggested that most extrapulmonary manifestations may be caused by disturbances in the adaptive immune response. Cellular and humoral immunity, including tissue-specific T cells and autoantibodies, may be involved in the pathogenesis of extrapulmonary manifestations of MP[29] . The results of this study showed that the occurrence of liver damage and cardiac enzyme profile abnormalities and pleural effusion was significantly higher in the mixed infection group than in the simple infection group in Hefei area. Therefore, the possibility of mixed infections is alerted to the occurrence of some complications in combination with the occurrence of some comorbidities in the children attending the clinic in Hefei area.
Our study has several limitations, first, the sample size was too small and from a single center, and also the condition of the children admitted to the hospital during the Mycoplasma pneumoniae outbreak may have been inherently more severe. These two points suggest some bias in our results. We acknowledge that our study may be subject to the inherent limitations of retrospective data collection and have taken steps to mitigate their impact. Selection bias was addressed by applying strict inclusion and exclusion criteria during participant/study selection. While retrospective designs have inherent limitations, we believe our rigorous methodology provides meaningful clinical insights.
Conclusion
In summary, this study found that during the outbreak of MP, the drug-resistant mutation rate of hospitalized children in Hefei was 100%, and that mixed infection of MRMP with other pathogens led to prolonged hospitalization and higher laboratory-related indicators in patients. In addition, there was an increased incidence of pleural effusion, hepatic impairment, and complications of abnormal cardiac enzyme profiles. This requires clinicians to pay close attention to the changes in the patient's disease during the course of treatment in order to prevent complications from affecting the quality of life of the child.
Abbreviations
Mycoplasma pneumoniae: MP, macrolide-resistant Mycoplasma pneumoniae: MRMP, Alanine aminotransferase: ALT, aspartate aminotransferase: AST, lactate dehydrogenase: LDH, creatine kinase: CK, platelet count: PLT, community-acquired pneumonia: CAP, refractory Mycoplasma pneumoniae pneumonia: RMPP, Mycoplasma pneumoniae pneumonia: MPP, Severe Acute Respiratory Syndrome Coronavirus 2: SARS-CoV-2, Coronavirus Disease 2019: COVID-19, Intensive Care Unit: ICU, white blood cell count: WBC, percentage of neutrophils: NEU, percentage of monocytes: MON, PLT, fibrinogen: FIB, prothrombin time: TT, D-dimer: DD, fibrinogen degradation product: FDP, urea: UREA, blood creatinine: CRE, blood uric acid: UA, glomerular filtration rate: eGFR, C-reactive protein: CRP, procalcitoninogen: PCT, activated partial thromboplastin time: APTT, prothrombin time: PT, total protein: TP, severe Mycoplasma pneumoniae pneumonia: SMPP, fulminant Mycoplasma pneumoniae pneumonia: FMPP, Epstein-Barr virus: EBV.
Declarations
Author Contributions
Zhengyuan Wang conceived the project and collect clinical data. Zhengyuan Wang performed data analysis and wrote the initial manuscript. Yuanhong Xu provided useful advice regarding the manuscript. All authors read and approved the final manuscript.
Acknowledgements
The authors thank the anonymous reviewers for their constructive comments. The authors are grateful to the medical staff in the First Affiliated Hospital of Anhui Medical University for their support in sample and clinical data collections.
Funding Information
This work was financially supported by Major Projects of Universities in Anhui Province (2022AH040162).
Ethics Approval and Consent to Participate
The current investigation was duly approved by the human ethics council of Anhui Medical University's First Affiliated Hospital (Approval No: Quick-PJ 2023-08-41). The written informed consent was obtained from patients in accordance with the Declaration of Helsinki.
Competing Interests
The authors declare that they have no existing or potential commercial or financial relationships that could create a conflict of interest at the time of conducting this study.
Data Availability
All data needed to evaluate the conclusions in the paper are present in the paper or the Supplementary Materials. Additional data related to this paper may be requested from the authors.
References
[1]Medjo B, Atanaskovic-Markovic M, Radic S, Nikolic D, Lukac M, Djukic S. Mycoplasma pneumoniae as a causative agent of community-acquired pneumonia in children: clinical features and laboratory diagnosis[J]. Italian Journal of Pediatrics, 2014, 40(1): 104. https://doi.org/10.1186/s13052-014-0104-4
[2]Zhao F, Li J, Liu J, Guan X, Gong J, Liu L, et al. Antimicrobial susceptibility and molecular characteristics of Mycoplasma pneumoniae isolates across different regions of China[J]. Antimicrobial Resistance & Infection Control, 2019, 8: 143. https://doi.org/10.1186/s13756-019-0576-5
[3]Lee H, Yun K W, Lee H J, Choi E H. Antimicrobial therapy of macrolide-resistant Mycoplasma pneumoniae pneumonia in children[J]. Expert Review of Anti-Infective Therapy, 2018, 16(1): 23-34. https://doi.org/10.1080/14787210.2018.1414599
[4]Norton S A. Diagnosing Mycoplasma pneumoniae-induced rash and mucositis (MIRM) in the emergency room[J]. Journal of the American Academy of Dermatology, 2015, 73(2): e67. https://doi.org/10.1016/j.jaad.2015.03.060
[5]Scapini J P, Flynn L P, Sciacaluga S, Morales L, Cadario M E. Confirmed Mycoplasma pneumoniae endocarditis[J]. Emerging Infectious Diseases, 2008, 14(10): 1664-1665. https://doi.org/10.3201/eid1410.080157
[6]Kawai Y, Miyashita N, Kubo M, Akaike H, Kato A, Nishizawa Y, et al. Therapeutic efficacy of macrolides, minocycline, and tosufloxacin against macrolide-resistant Mycoplasma pneumoniae in pediatric patients[J]. Antimicrobial Agents and Chemotherapy, 2013, 57(5): 2252-2258. https://doi.org/10.1128/AAC.00048-13
[7]Wang A, Wu Z, Huang Y, Zhou H, Wu L, Jia C P, et al. A 3D-printed microfluidic device for qPCR detection of macrolide-resistant mutations of Mycoplasma pneumoniae[J]. Biosensors, 2021, 11(11): 427. https://doi.org/10.3390/bios11110427
[8]Li F, Zhang Y, Shi P, Cao L, Su L, Fu P, et al. Mycoplasma pneumoniae and adenovirus coinfection cause pediatric severe community-acquired pneumonia[J]. Microbiology Spectrum, 2022, 10(2): e0002622. https://doi.org/10.1128/spectrum.00026-22
[9]Sung M, Choi H J, Lee M H, Lee J Y, Kim H B, Ahn Y M, et al. Regional and annual patterns in respiratory virus co-infection etiologies and antibiotic prescriptions for pediatric Mycoplasma pneumoniae pneumonia[J]. European Review for Medical and Pharmacological Sciences, 2022, 26(16): 5844-5856. https://doi.org/10.26355/eurrev_202208_29524
[10]Fan B E, Lim K G E, Chong V C L, Chan S S W, Ong K H, Kuperan P. COVID-19 and Mycoplasma pneumoniae coinfection[J]. American Journal of Hematology, 2020, 95(6): 723-724. https://doi.org/10.1002/ajh.25785
[11]Zha L, Shen J, Tefsen B, Wang Y, Lu W, Xu Q. Clinical features and outcomes of adult COVID-19 patients co-infected with Mycoplasma pneumoniae[J]. Journal of Infection, 2020, 81(3): e12-e15. https://doi.org/10.1016/j.jinf.2020.07.010
[12]Ni X. Community-acquired pneumonia diagnosis and treatment standard for children (2019 edition)[J]. Clinical and Education in Family Medicine, 2019, 17(9): 771-777. https://doi.org/10.13558/j.cnki.issn1672-3686.2019.09.002
[13]Matsuoka M, Narita M, Okazaki N, Ohya H, Yamazaki T, Ouchi K, et al. Characterization and molecular analysis of macrolide-resistant Mycoplasma pneumoniae clinical isolates obtained in Japan[J]. Antimicrobial Agents and Chemotherapy, 2004, 48(12): 4624-4630. https://doi.org/10.1128/AAC.48.12.4624-4630.2004
[14]De Francesco M A, Poiesi C, Gargiulo F, Bonfanti C, Pollara P, Fiorentini S, et al. Co-infection of chlamydia pneumoniae and Mycoplasma pneumoniae with SARS-CoV-2 is associated with more severe features[J]. Journal of Infection, 2021, 82(4): e4-e7. https://doi.org/10.1016/j.jinf.2021.01.009
[15]Xiong Y Z, He L M. Clinical analysis of infectious mononucleosis combined with Mycoplasma pneumoniae infection in children[J]. Journal of Nanchang University (Medical Edition), 2023, 63(5): 63-65, 74. https://doi.org/10.13764/j.cnki.ncdm.2023.05.011
[16]Shin S, Koo S, Yang Y J, Lim H J. Characteristics of the Mycoplasma pneumoniae epidemic from 2019 to 2020 in korea: macrolide resistance and Co-infection trends[J]. Antibiotics (Basel, Switzerland), 2023, 12(11): 1623. https://doi.org/10.3390/antibiotics12111623
[17]Poddighe D. Extra-pulmonary diseases related to Mycoplasma pneumoniae in children: recent insights into the pathogenesis[J]. Current Opinion in Rheumatology, 2018, 30(4): 380. https://doi.org/10.1097/BOR.0000000000000494
[18]Jiang X Y. Study on Mycoplasma pneumoniae infection and drug-resistant mutation in children in Guangyuan area[D]. Chuanbei Medical College, 2023. https://doi.org/10.27755/d.cnki.gcbyx.2023.000377
[19]Wu T. Study on the prevalence characteristics of Mycoplasma pneumoniae drug resistance genes and their correlation with genotypes in Yunnan[D]. Kunming University of Science and Technology, 2023. https://doi.org/10.27200/d.cnki.gkmlu.2023.001981
[20]Chen Y, Zhang Y, Tang Q N, Shi H B. Efficacy of doxycycline therapy for macrolide-resistant Mycoplasma pneumoniae pneumonia in children at different periods[J]. Italian Journal of Pediatrics, 2024, 50(1): 38. https://doi.org/10.1186/s13052-024-01615-y
[21]Kawakami N, Namkoong H, Saito F, et al. Epidemiology of macrolide-resistant Mycoplasma pneumoniae by age distribution in Japan[J]. Journal of Infection and Chemotherapy, 2021, 27(1): 45-48. https://doi.org/10.1016/j.jiac.2020.08.006
[22]Sauteur P M M, Chalker V J, Berger C, et al. Mycoplasma pneumoniae beyond the COVID-19 pandemic: where is it?[J]. The Lancet Microbe, 2022, 3(12): e897. https://doi.org/10.1016/S2666-5247(22)00190-2
[23]Chen Y, Tian W M, Chen Q, et al. Clinical characteristics and treatment of macrolide-resistant Mycoplasma pneumoniae pneumonia in children[J]. Chinese Journal of Contemporary Pediatrics, 2018, 20(8): 629-634. https://link.cnki.net/urlid/43.1301.R.20180807.1033.012
[24]Lee K Y, Lee H S, Hong J H, et al. Role of prednisolone treatment in severe Mycoplasma pneumoniae pneumonia in children[J]. Pediatric Pulmonology, 2006, 41(3): 263-268. https://doi.org/10.1002/ppul.20374
[25]Respiratory Group of Pediatric Branch of Chinese Medical Association, Editorial Committee of Chinese Journal of Applied Clinical Pediatrics. Expert consensus on diagnosis and treatment of Mycoplasma pneumoniae pneumonia in children (2015 edition)[J]. Chinese Journal of Applied Clinical Pediatrics, 2015, 30(17): 1304-1308. https://doi.org/10.3760/cma.j.issn.2095-428X.2015.17.006
[26]Hu T, Liang D A, Liu H Y. Characteristics and drug sensitivity analysis of Mycoplasma pneumoniae infection in children[J]. Guangdong Medical Journal, 2025(5). https://doi.org/10.13820/j.cnki.gdyx.20243514
[27]Liu Q, Meng H, Shan M F. Construction and validation of a nomogram diagnostic model for Mycoplasma pneumoniae combined with EB virus infection in children[J]. Chinese Journal of Nosocomiology, 2025(12): 1824-1828. https://kns.cnki.net/KCMS/detail/detail.aspx?dbcode=CAPJ&dbname=CAPJLAST&filename=ZHYY2025052600E
[28]Luo X Q, Luo J, Wang C J, Luo Z X, Tian D Y, Xie X H. Clinical features of severe Mycoplasma pneumoniae pneumonia with pulmonary complications in childhood: a retrospective study[J]. Pediatric Pulmonology, 2023, 58(10): 2815-2822. https://doi.org/10.1002/ppul.26593
[29]Fernald G W. Immunologic mechanisms suggested in the association of M. pneumoniae infection and extrapulmonary disease: a review[J]. Yale Journal of Biology and Medicine, 1983, 56(5-6): 475-479. https://pmc.ncbi.nlm.nih.gov/articles/PMC2590510/
 Figures
Figures References
References Peer
Peer Information
Information[1]Medjo B, Atanaskovic-Markovic M, Radic S, Nikolic D, Lukac M, Djukic S. Mycoplasma pneumoniae as a causative agent of community-acquired pneumonia in children: clinical features and laboratory diagnosis[J]. Italian Journal of Pediatrics, 2014, 40(1): 104. https://doi.org/10.1186/s13052-014-0104-4
[2]Zhao F, Li J, Liu J, Guan X, Gong J, Liu L, et al. Antimicrobial susceptibility and molecular characteristics of Mycoplasma pneumoniae isolates across different regions of China[J]. Antimicrobial Resistance & Infection Control, 2019, 8: 143. https://doi.org/10.1186/s13756-019-0576-5
[3]Lee H, Yun K W, Lee H J, Choi E H. Antimicrobial therapy of macrolide-resistant Mycoplasma pneumoniae pneumonia in children[J]. Expert Review of Anti-Infective Therapy, 2018, 16(1): 23-34. https://doi.org/10.1080/14787210.2018.1414599
[4]Norton S A. Diagnosing Mycoplasma pneumoniae-induced rash and mucositis (MIRM) in the emergency room[J]. Journal of the American Academy of Dermatology, 2015, 73(2): e67. https://doi.org/10.1016/j.jaad.2015.03.060
[5]Scapini J P, Flynn L P, Sciacaluga S, Morales L, Cadario M E. Confirmed Mycoplasma pneumoniae endocarditis[J]. Emerging Infectious Diseases, 2008, 14(10): 1664-1665. https://doi.org/10.3201/eid1410.080157
[6]Kawai Y, Miyashita N, Kubo M, Akaike H, Kato A, Nishizawa Y, et al. Therapeutic efficacy of macrolides, minocycline, and tosufloxacin against macrolide-resistant Mycoplasma pneumoniae in pediatric patients[J]. Antimicrobial Agents and Chemotherapy, 2013, 57(5): 2252-2258. https://doi.org/10.1128/AAC.00048-13
[7]Wang A, Wu Z, Huang Y, Zhou H, Wu L, Jia C P, et al. A 3D-printed microfluidic device for qPCR detection of macrolide-resistant mutations of Mycoplasma pneumoniae[J]. Biosensors, 2021, 11(11): 427. https://doi.org/10.3390/bios11110427
[8]Li F, Zhang Y, Shi P, Cao L, Su L, Fu P, et al. Mycoplasma pneumoniae and adenovirus coinfection cause pediatric severe community-acquired pneumonia[J]. Microbiology Spectrum, 2022, 10(2): e0002622. https://doi.org/10.1128/spectrum.00026-22
[9]Sung M, Choi H J, Lee M H, Lee J Y, Kim H B, Ahn Y M, et al. Regional and annual patterns in respiratory virus co-infection etiologies and antibiotic prescriptions for pediatric Mycoplasma pneumoniae pneumonia[J]. European Review for Medical and Pharmacological Sciences, 2022, 26(16): 5844-5856. https://doi.org/10.26355/eurrev_202208_29524
[10]Fan B E, Lim K G E, Chong V C L, Chan S S W, Ong K H, Kuperan P. COVID-19 and Mycoplasma pneumoniae coinfection[J]. American Journal of Hematology, 2020, 95(6): 723-724. https://doi.org/10.1002/ajh.25785
[11]Zha L, Shen J, Tefsen B, Wang Y, Lu W, Xu Q. Clinical features and outcomes of adult COVID-19 patients co-infected with Mycoplasma pneumoniae[J]. Journal of Infection, 2020, 81(3): e12-e15. https://doi.org/10.1016/j.jinf.2020.07.010
[12]Ni X. Community-acquired pneumonia diagnosis and treatment standard for children (2019 edition)[J]. Clinical and Education in Family Medicine, 2019, 17(9): 771-777. https://doi.org/10.13558/j.cnki.issn1672-3686.2019.09.002
[13]Matsuoka M, Narita M, Okazaki N, Ohya H, Yamazaki T, Ouchi K, et al. Characterization and molecular analysis of macrolide-resistant Mycoplasma pneumoniae clinical isolates obtained in Japan[J]. Antimicrobial Agents and Chemotherapy, 2004, 48(12): 4624-4630. https://doi.org/10.1128/AAC.48.12.4624-4630.2004
[14]De Francesco M A, Poiesi C, Gargiulo F, Bonfanti C, Pollara P, Fiorentini S, et al. Co-infection of chlamydia pneumoniae and Mycoplasma pneumoniae with SARS-CoV-2 is associated with more severe features[J]. Journal of Infection, 2021, 82(4): e4-e7. https://doi.org/10.1016/j.jinf.2021.01.009
[15]Xiong Y Z, He L M. Clinical analysis of infectious mononucleosis combined with Mycoplasma pneumoniae infection in children[J]. Journal of Nanchang University (Medical Edition), 2023, 63(5): 63-65, 74. https://doi.org/10.13764/j.cnki.ncdm.2023.05.011
[16]Shin S, Koo S, Yang Y J, Lim H J. Characteristics of the Mycoplasma pneumoniae epidemic from 2019 to 2020 in korea: macrolide resistance and Co-infection trends[J]. Antibiotics (Basel, Switzerland), 2023, 12(11): 1623. https://doi.org/10.3390/antibiotics12111623
[17]Poddighe D. Extra-pulmonary diseases related to Mycoplasma pneumoniae in children: recent insights into the pathogenesis[J]. Current Opinion in Rheumatology, 2018, 30(4): 380. https://doi.org/10.1097/BOR.0000000000000494
[18]Jiang X Y. Study on Mycoplasma pneumoniae infection and drug-resistant mutation in children in Guangyuan area[D]. Chuanbei Medical College, 2023. https://doi.org/10.27755/d.cnki.gcbyx.2023.000377
[19]Wu T. Study on the prevalence characteristics of Mycoplasma pneumoniae drug resistance genes and their correlation with genotypes in Yunnan[D]. Kunming University of Science and Technology, 2023. https://doi.org/10.27200/d.cnki.gkmlu.2023.001981
[20]Chen Y, Zhang Y, Tang Q N, Shi H B. Efficacy of doxycycline therapy for macrolide-resistant Mycoplasma pneumoniae pneumonia in children at different periods[J]. Italian Journal of Pediatrics, 2024, 50(1): 38. https://doi.org/10.1186/s13052-024-01615-y
[21]Kawakami N, Namkoong H, Saito F, et al. Epidemiology of macrolide-resistant Mycoplasma pneumoniae by age distribution in Japan[J]. Journal of Infection and Chemotherapy, 2021, 27(1): 45-48. https://doi.org/10.1016/j.jiac.2020.08.006
[22]Sauteur P M M, Chalker V J, Berger C, et al. Mycoplasma pneumoniae beyond the COVID-19 pandemic: where is it?[J]. The Lancet Microbe, 2022, 3(12): e897. https://doi.org/10.1016/S2666-5247(22)00190-2
[23]Chen Y, Tian W M, Chen Q, et al. Clinical characteristics and treatment of macrolide-resistant Mycoplasma pneumoniae pneumonia in children[J]. Chinese Journal of Contemporary Pediatrics, 2018, 20(8): 629-634. https://link.cnki.net/urlid/43.1301.R.20180807.1033.012
[24]Lee K Y, Lee H S, Hong J H, et al. Role of prednisolone treatment in severe Mycoplasma pneumoniae pneumonia in children[J]. Pediatric Pulmonology, 2006, 41(3): 263-268. https://doi.org/10.1002/ppul.20374
[25]Respiratory Group of Pediatric Branch of Chinese Medical Association, Editorial Committee of Chinese Journal of Applied Clinical Pediatrics. Expert consensus on diagnosis and treatment of Mycoplasma pneumoniae pneumonia in children (2015 edition)[J]. Chinese Journal of Applied Clinical Pediatrics, 2015, 30(17): 1304-1308. https://doi.org/10.3760/cma.j.issn.2095-428X.2015.17.006
[26]Hu T, Liang D A, Liu H Y. Characteristics and drug sensitivity analysis of Mycoplasma pneumoniae infection in children[J]. Guangdong Medical Journal, 2025(5). https://doi.org/10.13820/j.cnki.gdyx.20243514
[27]Liu Q, Meng H, Shan M F. Construction and validation of a nomogram diagnostic model for Mycoplasma pneumoniae combined with EB virus infection in children[J]. Chinese Journal of Nosocomiology, 2025(12): 1824-1828. https://kns.cnki.net/KCMS/detail/detail.aspx?dbcode=CAPJ&dbname=CAPJLAST&filename=ZHYY2025052600E
[28]Luo X Q, Luo J, Wang C J, Luo Z X, Tian D Y, Xie X H. Clinical features of severe Mycoplasma pneumoniae pneumonia with pulmonary complications in childhood: a retrospective study[J]. Pediatric Pulmonology, 2023, 58(10): 2815-2822. https://doi.org/10.1002/ppul.26593
[29]Fernald G W. Immunologic mechanisms suggested in the association of M. pneumoniae infection and extrapulmonary disease: a review[J]. Yale Journal of Biology and Medicine, 1983, 56(5-6): 475-479. https://pmc.ncbi.nlm.nih.gov/articles/PMC2590510/
Peer-review Terminology
Identity transparency: Single anonymized
Reviewer interacts with: Editor
Details
This is an open access article under the terms of the Creative Commons Attribution License(http://creativecommons.org/licenses/by/4.0/), which permits use, distribution and reproduction in any medium, provided the original work is properly cited.
Publication History
Received 2025-03-05
Accepted 2025-05-27
Published 2025-06-30