


Abstract
Background: Pulmonary fungal infection is a major risk factor for death and prolonged hospitalization in elderly patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD). At present, early recognition of these infections remains difficult. This study therefore collected clinical data to develop an early-prediction model for fungal pneumonia complicating AECOPD.
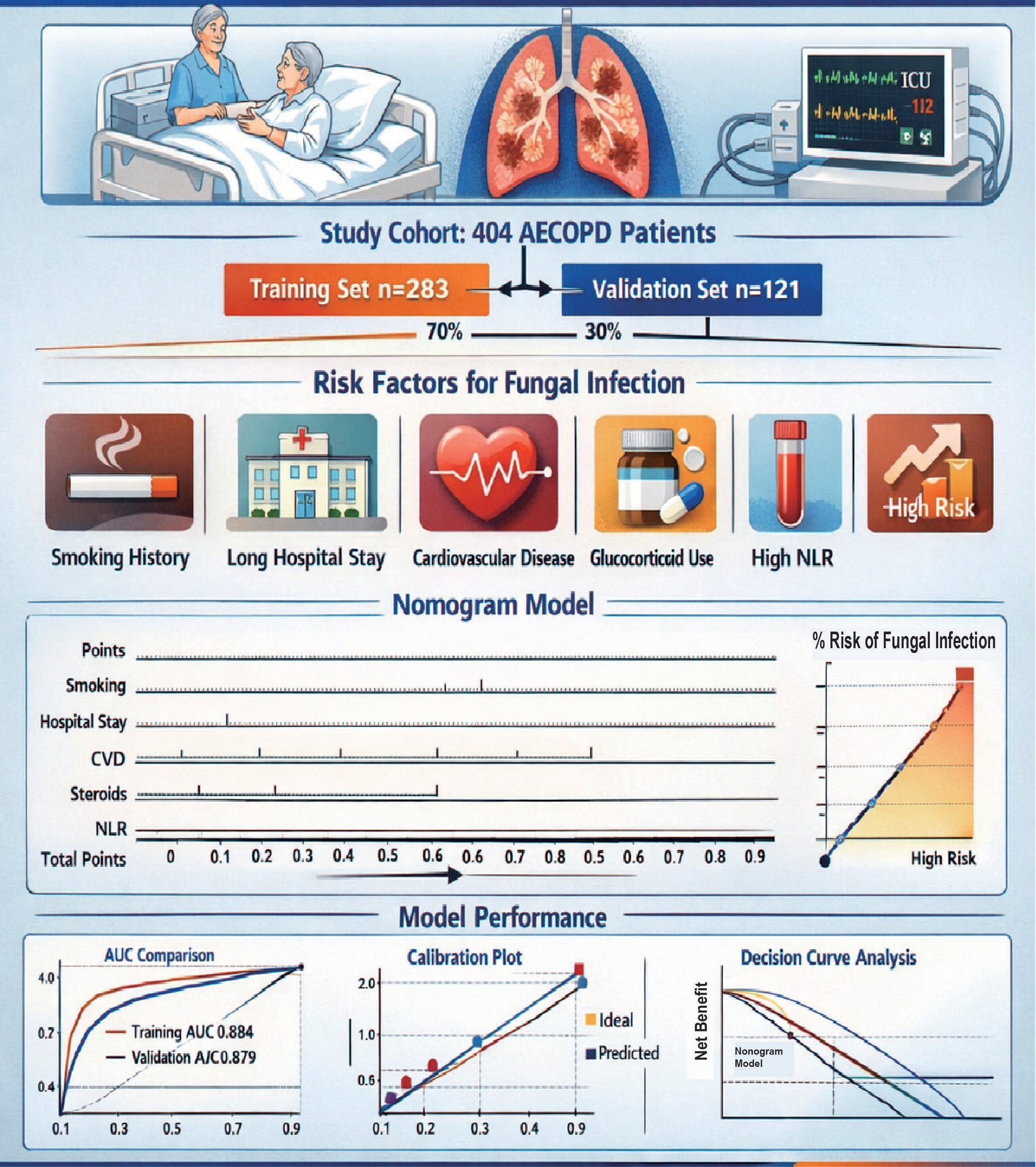
Methods: We enrolled 404 elderly AECOPD patients admitted to the Department of Respiratory Medicine, First Affiliated Hospital of Anhui Medical University, from January to December 2023. The cohort was randomly split 7:3 into a training set (n =283) and a validation set (n =121). Univariate logistic regression was first performed in the training set; variables with p < 0.05 were entered into a multivariate model. Significant factors were used to construct a nomogram. Model performance was evaluated in both sets by the area under the receiver operating characteristic curve (AUC), calibration plots, and decision-curve analysis (DCA).
Results: Smoking history, length of hospital stay, concomitant cardiovascular disease, glucocorticoid use, and the neutrophil-to-lymphocyte ratio (NLR) were independent risk factors for fungal infection during AECOPD (p < 0.05). The nomogram achieved AUCs of 0.884 [95% CI: 0.838–0.930] in the training set and 0.879 [95% CI: 0.795–0.962] in the validation set. Calibration and DCA curves indicated good clinical utility.
Conclusion: Smoking history, prolonged hospitalization, concurrent cardiovascular disease, glucocorticoid therapy, and elevated NLR are independent risk factors for fungal infection in AECOPD. The constructed nomogram exhibits strong predictive performance.
Keywords: elderly acute exacerbation of chronic obstructive pulmonary disease; fungal infection; risk factors; nomogram; prediction model
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous disorder characterised by chronic respiratory symptoms—dyspnoea, cough and sputum production with acute exacerbations—resulting from persistent abnormalities of the airways (bronchitis/bronchiolitis) and / or alveoli (emphysema) that lead to progressive, irreversible airflow limitation [1]. An acute exacerbation of COPD (AECOPD) is defined as a worsening of dyspnoea, cough and/or sputum within <14 days, often accompanied by tachypnoea or tachycardia and usually triggered by respiratory infection, air pollution or parenchymal injury; it is associated with intensified local and systemic inflammation. Elderly patients with COPD are intrinsically more fragile, and consequently more prone to super-imposed infection. Recent data rank COPD as the fourth leading cause of death worldwide [2]; its high prevalence, disability and mortality impose a heavy clinical burden and profoundly affect disease trajectory and prognosis [3]. Pulmonary fungal infection is largely opportunistic: fungi colonising the upper airways or other sites invade the lower respiratory tract when host immunity wanes, producing a spectrum of disease that ranges from mild respiratory symptoms to respiratory failure or septic shock [4]. Compared with other pulmonary disorders, AECOPD is accompanied by longer hospital stay, broader-spectrum antibiotic exposure and more frequent invasive procedures—all recognised risk factors for invasive mycosis [5]. Personalised prediction models that integrate multidimensional data have proved powerful in clinical risk stratification and are now widely used in contemporary medicine [6]. Although several independent risk factors for AECOPD complicated by pulmonary fungal infection have been identified, robust prognostic models remain scarce, especially for the elderly. Most previous studies have relied on single peripheral-blood indices; comprehensive models incorporating readily available inflammatory markers have rarely been reported. Against this background we sought to develop and validate a pragmatic prediction tool that quantifies the risk of concomitant fungal infection during hospitalisation in elderly patients with AECOPD, thereby facilitating timely empirical antifungal therapy and potentially improving clinical outcomes [7].
Study Population
A retrospective cohort design was adopted. From January to December 2023, 500 elderly
patients admitted to the Department of Respiratory Medicine, the First Affiliated Hospital of Anhui Medical
University, for acute exacerbation of chronic obstructive pulmonary disease (AECOPD) were consecutively screened.
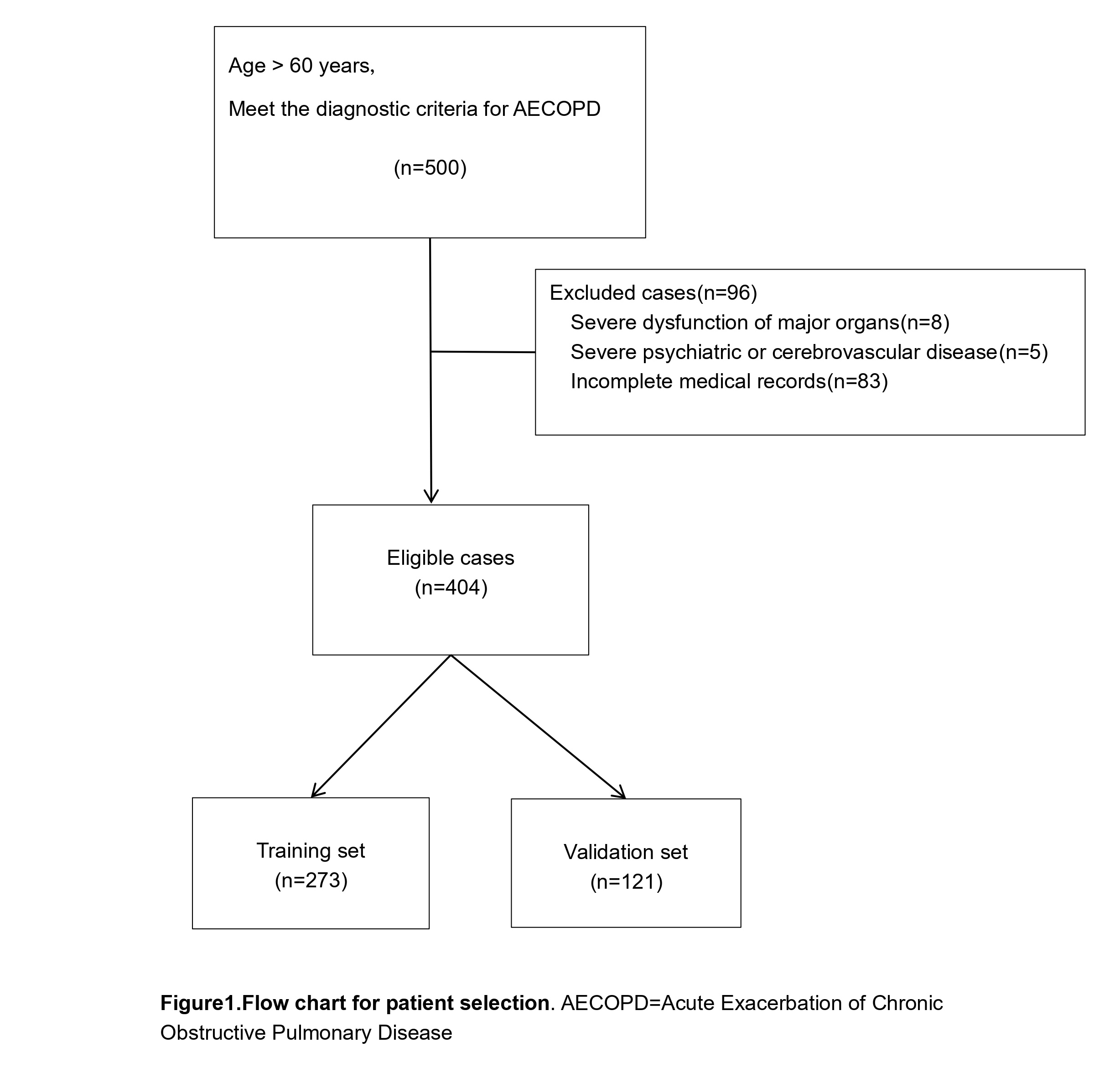
After application of inclusion and exclusion criteria, 404 cases were ultimately enrolled. The cohort was randomly
split into a training set (n = 283) and a validation set (n = 121) in a 7:3 ratio using a computer-generated
random-number sequence (Figure 1). The study protocol was approved by the Hospital Ethics Committee
approval (No. PJ-2025-01-18) and was conducted in accordance with the principles of the Declaration of Helsinki.
Figure 1. Flow chart of patient selection and cohort allocation for model development and validation. The diagram illustrates the derivation of the study population. Among 500 screened patients aged >60 years who met the diagnostic criteria for AECOPD, 96 were excluded (severe dysfunction of major organs, n=8; severe psychiatric or cerebrovascular disease, n=5; incomplete medical records, n=83). The remaining 404 eligible patients were randomly divided into a training set (n=283) for nomogram construction and a validation set (n=121) for internal validation.
Inclusion and Exclusion Criteria
Inclusion criteria: (1) Age greater than 60 years; (2) Patients
diagnosed with acute exacerbation of chronic obstructive pulmonary disease (AECOPD) according to the 2023 revised
Chinese expert consensus on the diagnosis and treatment of AECOPD [8] and confirmed by
spirometry.(4) Complete medical record.
Exclusion criteria:(1) Severe dysfunction of any major vital organ;(2) Severe psychiatric or cerebrovascular disease;(3) Insufficient clinical data.
Diagnostic Methodology for Fungal Infection
Diagnosis of fungal infection was based on the Expert
Consensus on the Diagnosis and Treatment of Pulmonary Mycoses issued by the Chinese Thoracic Society
[9] and Internal Medicine (9th Edition) [10], utilizing a three-tier diagnostic
classification system (proven, probable, possible). Diagnosis was determined by a comprehensive assessment of
clinical symptoms, imaging features, and microbiological findings in AECOPD patients. Suspected patients underwent
imaging studies, and sputum samples were collected. For patients with an initial positive fungal sputum culture, a
repeat sputum sample was collected for culture after 24-48 hours. Only cases with the same fungal species isolated
in two or more consecutive cultures were included in further analysis. Multiple sputum cultures showing mixed fungal
growth, in the absence of characteristic imaging changes or clinical symptom exacerbation, were considered
contaminated and excluded. For patients with positive fungal sputum cultures but lacking definitive clinical symptoms
or imaging evidence of pulmonary infection, antifungal treatment response was evaluated: cases were classified as
fungal colonisation (and excluded from the infection group) if there was no symptom progression or imaging
deterioration without antifungal therapy, or if no improvement was observed following antifungal treatment. Only
cases demonstrating clinical and radiological improvement in response to antifungal therapy were confirmed as
pulmonary fungal infections.
Data collection
Baseline characteristics and comorbidities were systematically extracted from the electronic
medical record, including age, sex, Body Mass Index (BMI), smoking history, alcohol consumption, and co-existing
conditions such as hypertension, diabetes mellitus, and cardiovascular disease. The initial clinical presentation,
physical findings, and the first available laboratory results obtained after admission were also recorded. Throughout
hospitalization, all therapeutic interventions—specifically the administration of systemic corticosteroids and
antimicrobial agents, as well as the use or non-use of mechanical ventilation—were prospectively logged. Clinical
outcomes were subsequently evaluated in terms of total length of stay and the occurrence of in-hospital death.
Statistical analysis
All data processing, inferential statistics, and visualizations were performed with
SPSS 27.0 and R 4.5.1. Two-sided tests were used throughout; statistical significance was set at P < 0.05.
Continuous variables were first examined for normality. Normally distributed data are presented as mean ± SD (x̅ ± s);
non-normally distributed data are expressed as median [inter-quartile range, M (Q1, Q3)]. The entire cohort was
randomly split 7:3, yielding a training set (n = 283) and a validation set (n = 121). In the training set,
univariable logistic regression was applied to screen variables; those with p < 0.05 were entered into a
multivariable logistic model. Significant predictors retained in the final model were used to construct a nomogram.
Model performance was evaluated in both the training and validation sets with ROC curves, calibration plots, and
decision-curve analysis (DCA).
Baseline characteristics of elderly patients presenting with acute exacerbation of chronic obstructive pulmonary
disease and co-existing pulmonary fungal infections
A total of 404 patients were enrolled, including 311
males (77.0 %) and 93 females (23.0 %); 105 individuals (26.0 %) constituted the fungal-infection group
(Table 1). Among the 105 patients with pulmonary fungal co-infection, Aspergillus fumigatus was the
leading pathogen (n = 46, 43.8 %), followed by Candida albicans (n = 24, 22.9 %), Aspergillus flavus (n = 6,
5.7 %), Aspergillus niger (n = 5, 4.8%), Aspergillus sydowii (n = 1, 0.95 %), and Candida tropicalis (n = 1,
0.95 %); the causative organism remained unidentified in 22 cases (21.0 %). Among them, confirmed infections (83
cases, accounting for 79.0%) were diagnosed based on: (a) confirmation by histopathological examination, or (b)
clinical manifestations consistent with infection, along with the same fungus detected in two or more consecutive
sputum or bronchoalveolar lavage fluid cultures. Clinically diagnosed infections (22 cases, accounting for 21.0%,
the "causative organism remained unidentified" group). These patients met all the following diagnostic criteria:
although the specific pathogen could not be identified through consecutive cultures or histopathological examination,
the diagnosis was established based on sufficient clinical, imaging, and indirect laboratory evidence. This study,
adhering to the rigor of the predictive model, excluded suspected cases. That is, patients who only met the criteria
for host factors combined with clinical or imaging features but lacked any mycological evidence (direct or indirect)
were not included. The mean age was 75.97 years in the infection group versus 74.20 years in the non-infected group.
Fever on admission was observed in 25.7 % of the fungal-infection group compared with 16.7 % of those without
infection. Current or former smokers were more prevalent in the infected cohort (53.5 % and 37.1 %). Median length
of stay was longer for infected patients (13 days and 10.25 days). Systemic corticosteroids were administered to
69.5 % of the infected group but only 13.7 % of the non-infected group, and antibiotic duration was likewise
extended in the former. Mean BMI was lower in infected individuals (19.43 kg/m² and 23.92 kg/m²). Comorbid
hypertension was reported in 42.9 % of infected and 47.1 % of non-infected patients; corresponding figures for
diabetes were 18.1 % and 13.7 %, and for cardiovascular disease 52.4 % and 38.5 %.
Table 1. Baseline characteristics of elderly patients presenting with acute exacerbation of chronic obstructive pulmonary disease and co-existing pulmonary fungal infections.
| Variable | Total (n=404) | Fungal Infection (n=105) | Without Fungal Infection (n=299) | χ²/t | P-value |
|---|---|---|---|---|---|
| Age, years | 74.8±9.70 | 75.97±9.42 | 74.23±9.79 | -1.61 | 0.110 |
| Fever | 77(19.1%) | 27(25.7%) | 50(16.7%) | 3.51 | 0.06 |
| Hypertension | 186(46.0%) | 45(42.9%) | 141(47.1%) | 0.5 | 0.479 |
| Diabetes Mellitus | 60(14.9%) | 19(18.1%) | 41(13.7%) | 0.86 | 0.354 |
| Cardiovascular Disease | 152(37.6%) | 55(52.4%) | 97(38.5%) | 12.85 | <0.001 |
| Smoking history | 167(41.3%) | 56(53.3%) | 111(37.1%) | 7.77 | 0.05 |
| BMI (kg/m²) | 22.7 ± 16.0 | 19.43±6.64 | 23.92±18.24 | 2.08 | 0.05 |
| Length of Hospital Stay, days | 10.96 ± 7.91 | 13.00±12.28 | 10.25±5.63 | -2.20 | 0.030 |
| Duration of Glucocorticoid Use | 114(28.2%) | 73(69.5%) | 41(13.7%) | 11.67 | <0.001 |
| WBC, ×10⁹/L | 8.86 ± 4.22 | 10.75±5.75 | 8.19±3.54 | -4.28 | <0.001 |
| NLR | 10.33 ± 19.82 | 17.82±35.35 | 7.70±9.69 | -2.87 | 0.01 |
| CRP, mg/L | 36.62 ± 56.1 | 45.18±59.63 | 33.62±54.85 | -1.75 | 0.08 |
| ALB, g/L | 36.38 ± 5.44 | 35.63±5.53 | 36.64±5.41 | 1.62 | 0.11 |
| PA, mg/L | 164.5 ± 73.9 | 127.65±82.64 | 177.39±70.54 | 4.30 | <0.001 |
| Glu, mmol/L | 6.95 ± 2.59 | 7.48±3.23 | 6.76±2.33 | -2.08 | 0.04 |
Pulmonary Fungal Infection in Elderly Patients Hospitalized for Acute Exacerbation of Chronic Obstructive Pulmonary Dis-ease
Univariable analysis of the training cohort revealed
statistically significant differences (p < 0.05) between patients with and without concomitant fungal infection in
the following variables: presence of fever, smoking history, length of hospital stay, co-existing cardiovascular
disease, systemic corticosteroid use, duration of corticosteroid therapy, white-blood-cell count,
neutrophil-to-lymphocyte ratio (NLR), C-reactive protein level, and blood glucose concentration. No significant
differences were observed for any other parameters (p > 0.05) (Table 2).
Table 2. Univariable Analysis of Risk Factors for Pulmonary Fungal Infection in Elderly Patients Hospitalized for Acute Exacerbation of Chronic Obstructive Pulmonary Disease.
| Variable | OR-value | 95%CI | P-value |
|---|---|---|---|
| Age, years | 1.003 | 0.998~1.009 | 0.256 |
| Gender, Male; Female | 0.949 | 0.839~1.074 | 0.410 |
| Fever | 1.227 | 1.083~1.39 | 0.001 |
| Hypertension | 0.939 | 0.846~1.042 | 0.240 |
| Diabetes Mellitus | 1.054 | 0.908~1.224 | 0.492 |
| Cardiovascular Disease | 1.131 | 1.016~1.258 | 0.025 |
| Smoking history | 1.194 | 1.077~1.323 | 0.001 |
| BMI (kg/m²) | 1.000 | 0.994~1.006 | 0.996 |
| Length of Hospital Stay, days | 1.007 | 1.001~1.013 | 0.017 |
| Duration of antibiotic therapy, days | 1.003 | 0.996~1.01 | 0.351 |
| Duration of Glucocorticoid Use | 1.663 | 1.509~1.834 | <0.001 |
| Duration of Glucocorticoid Use, days | 1.007 | 1.001~1.013 | 0.015 |
| WBC, ×10⁹/L | 1.026 | 1.015~1.037 | <0.001 |
| NLR | 1.008 | 1.005~1.01 | <0.001 |
| CRP, mg/L | 0.987 | 0.977~0.997 | 0.011 |
| ALB, g/L | 1.000 | 1.000 | 0.107 |
| PA, mg/L | 0.858 | 0.735~1.002 | 0.054 |
| Glu, mmol/L | 1.399 | 1.209~1.619 | <0.001 |
Multivariable logistic regression analysis of risk factors for pulmonary fungal infection in elderly patients with
acute exacerbation of chronic obstructive pulmonary disease
Multivariable logistic regression—using fungal
infection as the dependent variable and all factors with p < 0.05 in Table 2 as
covariates—identified smoking history, length of hospital stay, co-existing cardiovascular disease, systemic
corticosteroid use, and NLR as independent predictors (all p < 0.05) (Table 3).
Table 3. Multivariable logistic regression analysis of risk factors for pulmonary fungal infection in elderly patients with acute exacerbation of chronic obstructive pulmonary disease.
| Variable | OR-value | 95%CI | P-value |
|---|---|---|---|
| Smoking history | 1.194 | 1.077~1.323 | 0.001 |
| Length of Hospital Stay | 1.007 | 1.001~1.013 | 0.017 |
| Cardiovascular Disease | 1.131 | 1.016~1.258 | 0.025 |
| Systemic glucocorticoid therapy | 1.663 | 1.509~1.834 | <0.001 |
| NLR | 1.008 | 1.005~1.01 | <0.001 |
Prediction Model Development
Based on the multivariable logistic regression coefficients, the five
independent risk factors (smoking history, length of hospital stay, concomitant cardiovascular disease, systemic
corticosteroid use, and NLR) were each weighted and assigned corresponding points. Summing the points for an
individual patient and locating the total on the lower axis of the nomogram yields the predicted probability of
fungal infection (Figure 2). ROC curves (Figure 3) were nearly superimposable
between the training and validation sets, with areas under the curve (AUC) of 0.884 [95% CI 0.838–0.930] and 0.879
[95% CI 0.796–0.962], respectively. Calibration plots (Figure 4) showed close agreement between
predicted probabilities and observed event rates; Hosmer-Lemeshow tests yielded p > 0.05 in both cohorts.
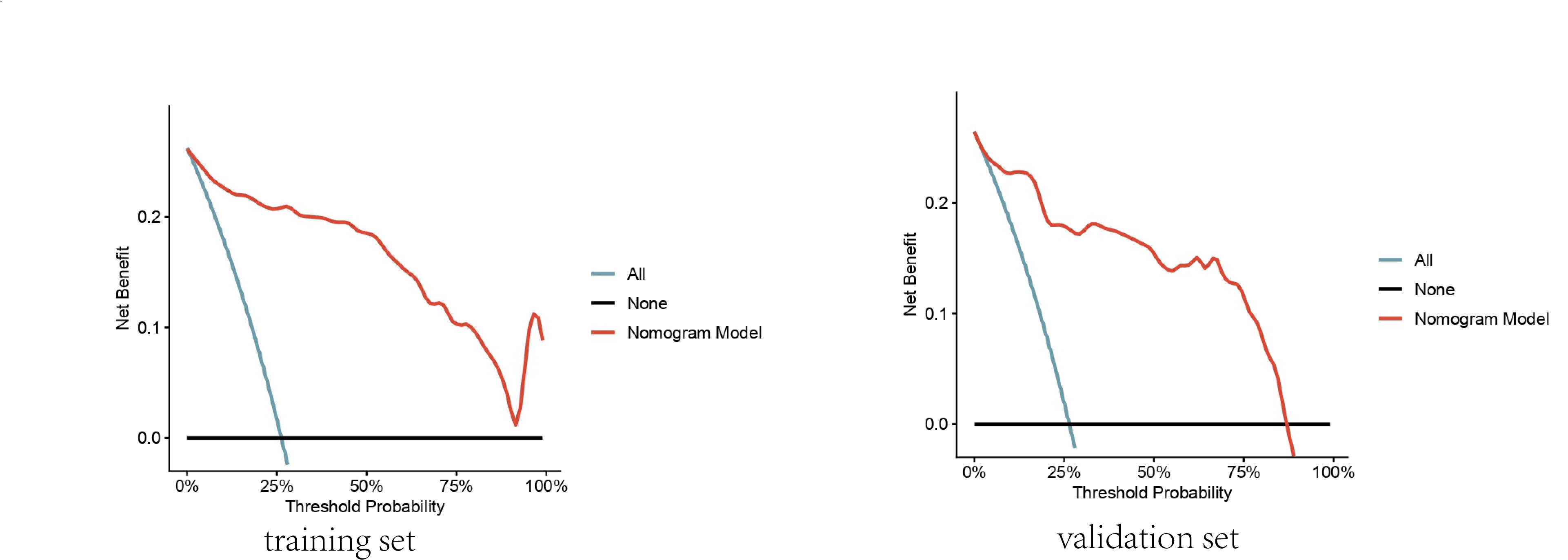
Decision-curve analysis (DCA, Figure 5) demonstrated favorable net clinical benefit across the full
range of reasonable threshold probabilities.
Figure 2. Nomogram predicting the probability of pulmonary fungal infection in elderly patients hospitalized for AECOPD. The model incorporates five independent risk factors identified by multivariable logistic regression: Systemic glucocorticoid therapy (yes = 1, no = 0), Neutrophil-to-lymphocyte ratio (NLR, continuous), Smoking history (yes = 1, no = 0), Length of hospital stay (days, continuous), Cardiovascular disease (yes = 1, no = 0). To obtain the predicted probability: Locate the patient's value on each variable axis → draw a vertical line up to the "Points" axis to determine points for that variable. Sum the points for all variables → locate the total on the "Total Points" axis. Drop a vertical line from the total-points value to the "Predicted value of infection" axis to read the probability (0–1).
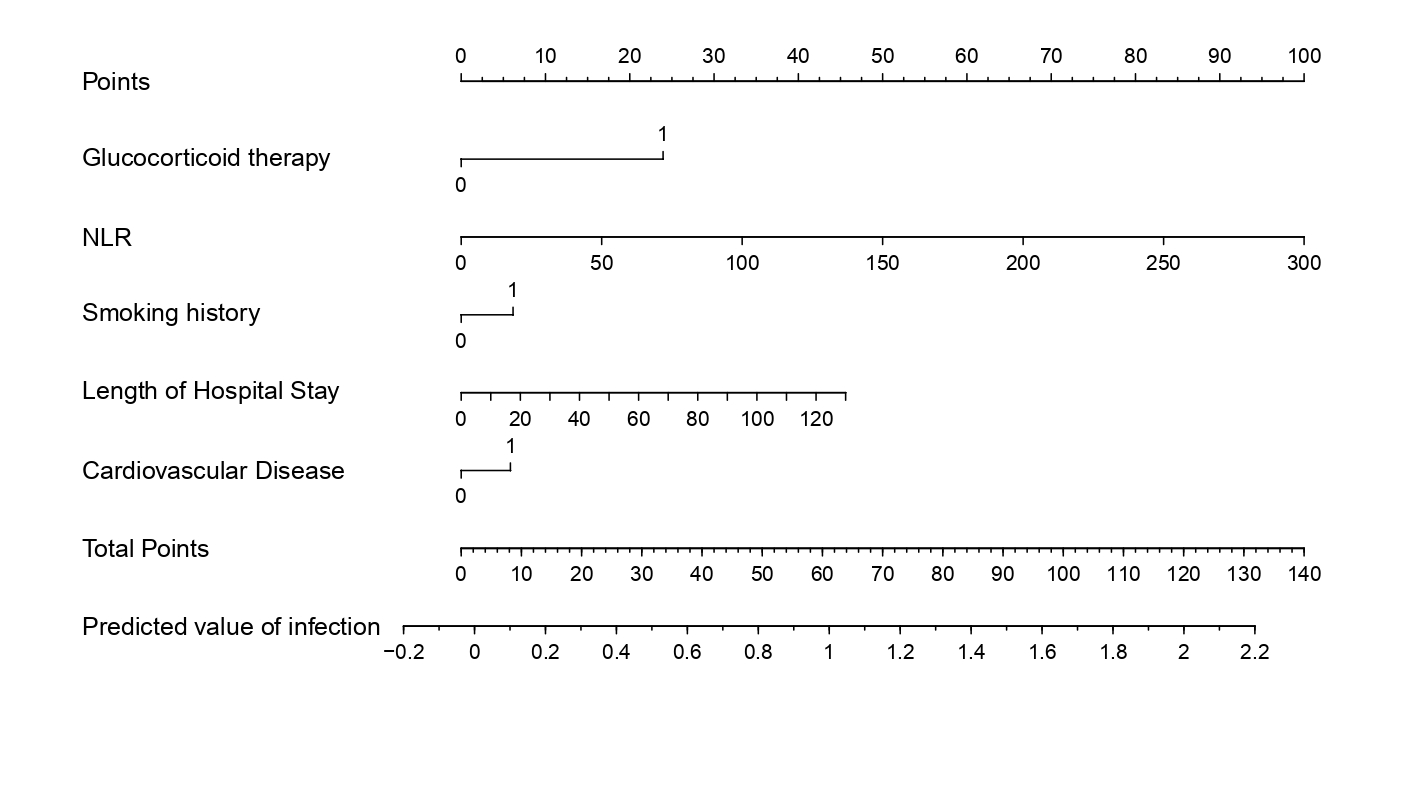
Figure 3. ROC curves of the nomogram for predicting pulmonary fungal infection in elderly AECOPD patients. The diagram displays the receiver operating characteristic (ROC) curves for both the training set and the validation set. Training set: AUC = 0.884 (95 % CI 0.838–0.930). Validation set: AUC = 0.879 (95 % CI 0.795–0.962). Statistical methods: ROC analysis was performed with the pROC package in R 4.5.1; 95 % confidence intervals were calculated by 2,000 bootstrap replications.
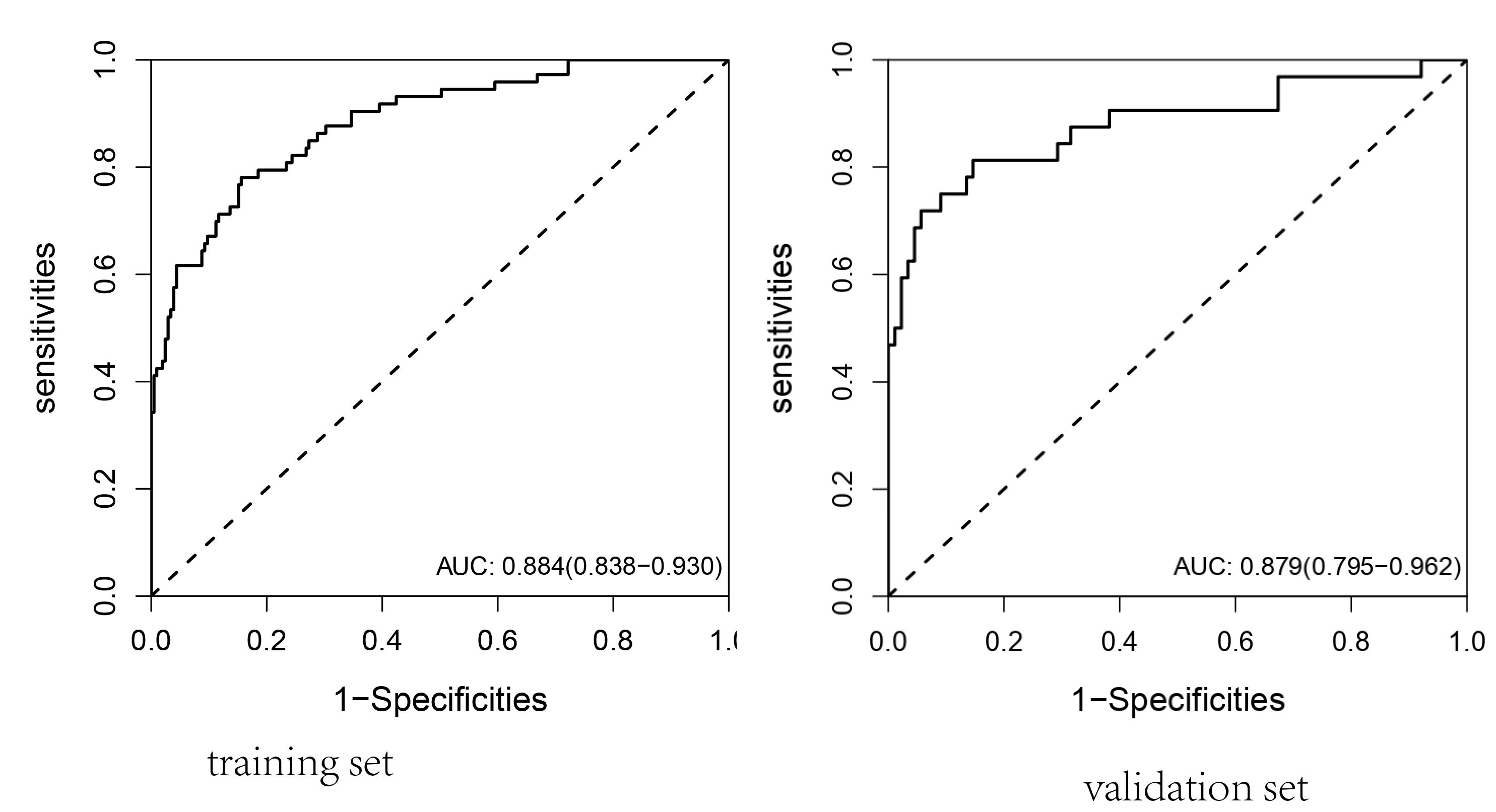
Figure 4. Calibration plots of the nomogram for predicting the probability of pulmonary fungal infection in elderly AECOPD patients. The left and right panels display the agreement between predicted and observed probabilities in the training and validation sets, respectively. The diagonal gray dashed line represents perfect calibration (Ideal). The solid lines show the apparent (raw) calibration, while the dashed lines (Bias-corrected) are adjusted for overfitting using 1,000 bootstrap resamples. Points or curves closer to the Ideal line indicate better calibration.
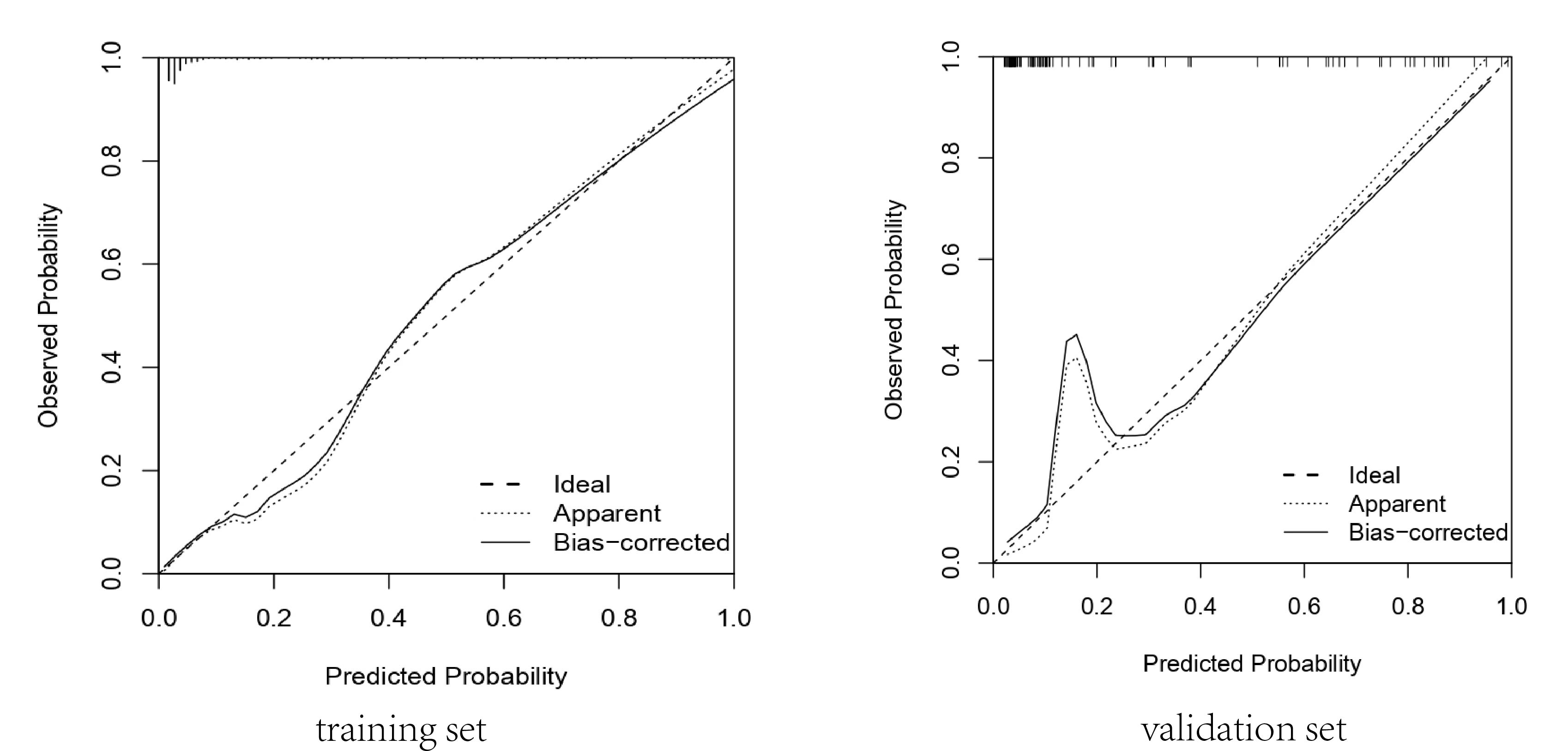
Figure 5. Decision curve analysis (DCA) for the nomogram predicting pulmonary fungal infection in elderly AECOPD patients. The left and right panels display threshold probability versus net benefit curves for the training and validation sets, respectively. The blue "All" line assumes all patients are infected and treated; the gray "None" line assumes no treatment; the red "Nomogram Model" line represents the net clinical benefit of using the nomogram to guide treatment decisions. Across clinically relevant threshold probabilities (0–25%), the model maintains a positive net benefit, indicating superior clinical utility compared to treating all or no patients. Statistical methods: DCA was performed using the rmda package in R version 4.5.1; net benefit was calculated with 1,000 bootstrap resamples for bias correction.
Discussion
COPD is a heterogeneous disorder. GOLD 2025 classifies its determinants into genetic susceptibility, environmental exposures and events occurring across the life-course; together these insults destroy lung parenchyma and distort normal lung development or ageing [1]. Acute exacerbations are frequently complicated by co-morbidities that further depress systemic immunity and predispose to secondary fungal infection. In the present series 105 of 404 eligible patients (26.0 %) acquired pulmonary mycoses, with Aspergillus spp. predominating—a distribution consistent with previous reports. Multivariable analysis identified five independent risk factors: current or past smoking, prolonged hospital stay, concomitant cardiovascular disease, systemic corticosteroid therapy and an elevated neutrophil-to-lymphocyte ratio (NLR).
Smoking increases the risk of pulmonary fungal infection
Cigarette smoke exerts broad immunosuppressive
effects. Nicotine, tar and other combustion products impair mucociliary clearance, damage airway epithelium and blunt
phagocytic activity of alveolar macrophages and neutrophils while suppressing T- and B-cell responses
[11]. These defects compromise respiratory barrier function and facilitate fungal colonisation and
invasion, particularly during exacerbations when airway inflammation is most intense. The human respiratory tract
harbors a complex ecosystem composed of bacteria, fungi, and viruses. Disruptions within this microbial community are
closely associated with the onset and progression of various respiratory diseases. When the airways are exposed to
external stimuli, the host mounts an abnormal immune response accompanied by persistent inflammation, which in turn
reshapes the composition and structure of the airway microbiota. Smoking disrupts this ecological balance to some
extent [12]. Our data confirm that smoking significantly increases the risk of invasive fungal
disease in elderly AECOPD patients.
Prolonged hospital stay is a risk factor for co-existing pulmonary fungal infection
Length of hospital
stay is a proxy for cumulative exposure to antibiotics, corticosteroids and invasive procedures such as
intubation—each of which disrupts mechanical or immunological defences. We observed a direct relationship between
duration of admission and probability of fungal infection, underscoring the need for heightened surveillance in
long-stay patients. Prolonged hospitalization not only prolongs exposure to broad-spectrum antibiotics and invasive
devices but also intensifies physiological stress and immunosuppression, all of which synergistically amplify the
risk profile; consequently, the likelihood of acquiring pulmonary fungal infection rises substantially, especially in
elderly or nutritionally depleted individuals.
Systemic corticosteroid use significantly increases the risk of pulmonary fungal infection
Systemic
corticosteroids, while dampening harmful inflammation, simultaneously impair cell-mediated immunity. Experimental
work demonstrates that glucocorticoids directly enhance fungal growth, morphological switching and virulence-factor
expression in Aspergillus and Candida spp [13-15]. In our cohort, both
corticosteroid use and longer courses were strongly associated with mycotic infection.
Finally, repeated or broad-spectrum antibiotic therapy eradicates bacterial competitors and allows fungal overgrowth [16]. We found that every additional day of antibiotic treatment incrementally increased infection odds, emphasising the importance of stringent antimicrobial stewardship in AECOPD management.
Co-existing cardiovascular disease is an independent risk factor for pulmonary fungal infection in AECOPD
patients
The circulatory disorders enrolled in this study included coronary artery disease, chronic heart
failure, valvular heart disease, and related conditions. The three most frequent cardiac comorbidities in COPD are
atrial fibrillation (AF), heart failure (HF), and ischaemic heart disease (IHD), all of which—like COPD—present
chiefly with dyspnoea. HF intensifies the respiratory symptoms of AECOPD by producing pulmonary congestion, airway
oedema and reduced exercise tolerance; it also disrupts the mucosal mechanical barrier, creating favourable
conditions for fungal colonisation. Cardiovascular disease and fungal infection share common risk factors such as
advanced age, smoking and diabetes. Conversely, the marked systemic inflammation during AECOPD increases the risk of
acute coronary events, generating a "fungal infection–HF" vicious circle. Shared pathophysiological
substrates—oxidative stress, endothelial dysfunction and immunosenescence—make cardiovascular disease the second
leading cause of death in COPD patients with pulmonary disorders [17, 18].
A higher neutrophil-to-lymphocyte ratio (NLR) is associated with an increased probability of pulmonary fungal
infection in elderly AECOPD patients
Leukocytosis disrupts immune homeostasis by creating an inflammatory
milieu in which pro-inflammatory cytokines suppress anti-fungal immunity. Bacterial super-infection triggers massive
neutrophil recruitment and exuberant release of cytokines that impair macrophage-mediated killing of Aspergillus and
Candida spp. The neutrophil-to-lymphocyte ratio (NLR), a composite inflammatory index derived from routine full
blood count, offers rapid, inexpensive and reproducible quantification of this dysregulated response. In the present
study, elevated NLR emerged as an independent risk factor for fungal infection in AECOPD. Previous work has shown
that high NLR correlates with impaired pulmonary ventilation in exacerbated COPD, presumably by amplifying airway
inflammation and parenchymal damage, thereby facilitating fungal colonisation and invasion
[19].
Studies also show that serum albumin reflects overall nutritional reserve; lower concentrations indicate malnutrition, which negatively influences both survival and long-term prognosis [17, 20]. Albumin itself maintains colloid oncotic pressure, transports endogenous and exogenous solutes (hormones, free fatty acids, drugs), and functions as a nitrogen reserve and acid–base buffer; its serum level is a central biochemical index of nutritional status, hepatic function, and systemic inflammation [21]. Chronic dysglycaemia induces systemic microangiopathy, reduces alveolar–capillary oxygen diffusion, and disrupts pulmonary parenchymal architecture—changes that collectively facilitate invasive fungal colonisation [22]. Additionally, elevated blood glucose exacerbates endothelial dysfunction [23], further compromising respiratory function and amplifying the likelihood of fungal infection. In this study, low protein levels and elevated blood glucose were also identified as risk factors for AECOPD complicated with pulmonary fungal infection. Although they were not included in the final predictive model, this may be attributed to the small sample size. Therefore, these two indicators also warrant additional attention in clinical practice.
Although the present study did not identify radiological features such as emphysema, bullae or old tuberculosis scars as independent risk factors, earlier reports have consistently linked these structural abnormalities to pulmonary mycosis. Whether their non-significance in our cohort reflects a true absence of effect or is attributable to limited statistical power remains uncertain; enlarging the sample size in future investigations will be necessary to clarify their contribution [24].
In addition, the single-centre, retrospective design inevitably introduces selection and information bias; future work should adopt prospective, multicentre protocols to enhance external validity and robustness.
Conclusion
In summary, pulmonary fungal infection is common in elderly patients hospitalized for AECOPD and is associated with poor outcomes. Early recognition is therefore essential. Smoking history, prolonged length of stay, pre-existing cardiovascular disease, systemic corticosteroid use (and its duration), and elevated NLR are independent correlates of mycotic complications. Clinicians should maintain a high index of suspicion for invasive fungal disease when any of these factors are present in an elderly AECOPD inpatient.
Abbreviations
AECOPD - Acute Exacerbation of Chronic Obstructive Pulmo-nary Disease; AF - Atrial Fibrillation; ALB - Albumin; AUC - Area Under the Curve; COPD - Chronic Obstructive Pulmonary Dis-ease; CRP - C-Reactive Protein; DCA - Decision Curve Analysis; HF - Heart Failure; IHD - Ischaemic Heart Disease ; NLR - Neu-trophil-to-Lymphocyte Ratio; PA - Prealbumin; ROC - Receiver Operating Characteristic; WBC - White Blood Cell.
Declarations
Author contributions
Tiantian Zhang: Writing, review, editing, Writing, original draft, Conceptualization, Visualization, Formal analysis, Data curation. Siyu Sun: Writing, review, editing, Validation, Supervision, Data curation, Formal analysis. Yingying Zhu: Writing – review, editing, Conceptualization, Supervision. All authors read and approved the final manuscript.
Acknowledgements
Not applicable.
Funding information
This work was supported by the National Natural Science Foundation of China Youth Science Fund Cultivation Program (Grant No. 2019kj05).
Ethics approval and consent to participate
The study protocol was approved by the Hospital Ethics Committee approval (No. PJ-2025-01-18).
Competing Interests
The authors declare that they have no existing or potential commercial or financial relationships that could create a conflict of interest at the time of conducting this study.
Data availability
Not applicable.
References
[10] Junbo G, Yongjian X, Chen W. Internal Medicine, 9th Edition. Beijing: People's Medical Publishing House.
 Figures
Figures References
References Peer
Peer Information
InformationFigure 1. Flow chart of patient selection and cohort allocation for model development and validation. The diagram illustrates the derivation of the study population. Among 500 screened patients aged >60 years who met the diagnostic criteria for AECOPD, 96 were excluded (severe dysfunction of major organs, n=8; severe psychiatric or cerebrovascular disease, n=5; incomplete medical records, n=83). The remaining 404 eligible patients were randomly divided into a training set (n=283) for nomogram construction and a validation set (n=121) for internal validation.
Figure 2. Nomogram predicting the probability of pulmonary fungal infection in elderly patients hospitalized for AECOPD. The model incorporates five independent risk factors identified by multivariable logistic regression: Systemic glucocorticoid therapy (yes = 1, no = 0), Neutrophil-to-lymphocyte ratio (NLR, continuous), Smoking history (yes = 1, no = 0), Length of hospital stay (days, continuous), Cardiovascular disease (yes = 1, no = 0). To obtain the predicted probability: Locate the patient's value on each variable axis → draw a vertical line up to the "Points" axis to determine points for that variable. Sum the points for all variables → locate the total on the "Total Points" axis. Drop a vertical line from the total-points value to the "Predicted value of infection" axis to read the probability (0–1).
Figure 3. ROC curves of the nomogram for predicting pulmonary fungal infection in elderly AECOPD patients. The diagram displays the receiver operating characteristic (ROC) curves for both the training set and the validation set. Training set: AUC = 0.884 (95 % CI 0.838–0.930). Validation set: AUC = 0.879 (95 % CI 0.795–0.962). Statistical methods: ROC analysis was performed with the pROC package in R 4.5.1; 95 % confidence intervals were calculated by 2,000 bootstrap replications.
Figure 4. Calibration plots of the nomogram for predicting the probability of pulmonary fungal infection in elderly AECOPD patients. The left and right panels display the agreement between predicted and observed probabilities in the training and validation sets, respectively. The diagonal gray dashed line represents perfect calibration (Ideal). The solid lines show the apparent (raw) calibration, while the dashed lines (Bias-corrected) are adjusted for overfitting using 1,000 bootstrap resamples. Points or curves closer to the Ideal line indicate better calibration.
Figure 5. Decision curve analysis (DCA) for the nomogram predicting pulmonary fungal infection in elderly AECOPD patients. The left and right panels display threshold probability versus net benefit curves for the training and validation sets, respectively. The blue "All" line assumes all patients are infected and treated; the gray "None" line assumes no treatment; the red "Nomogram Model" line represents the net clinical benefit of using the nomogram to guide treatment decisions. Across clinically relevant threshold probabilities (0–25%), the model maintains a positive net benefit, indicating superior clinical utility compared to treating all or no patients. Statistical methods: DCA was performed using the rmda package in R version 4.5.1; net benefit was calculated with 1,000 bootstrap resamples for bias correction.
[10] Junbo G, Yongjian X, Chen W. Internal Medicine, 9th Edition. Beijing: People's Medical Publishing House.
Peer-review Terminology
Identity transparency: Single anonymized
Reviewer interacts with: Editor
Details
This is an open access article under the terms of the Creative Commons Attribution License(http://creativecommons.org/licenses/by/4.0/), which permits use, distribution and reproduction in any medium, provided the original work is properly cited.
Publication History
Received 2025-12-05
Accepted 2026-02-13
Published 2026-03-08