


Abstract
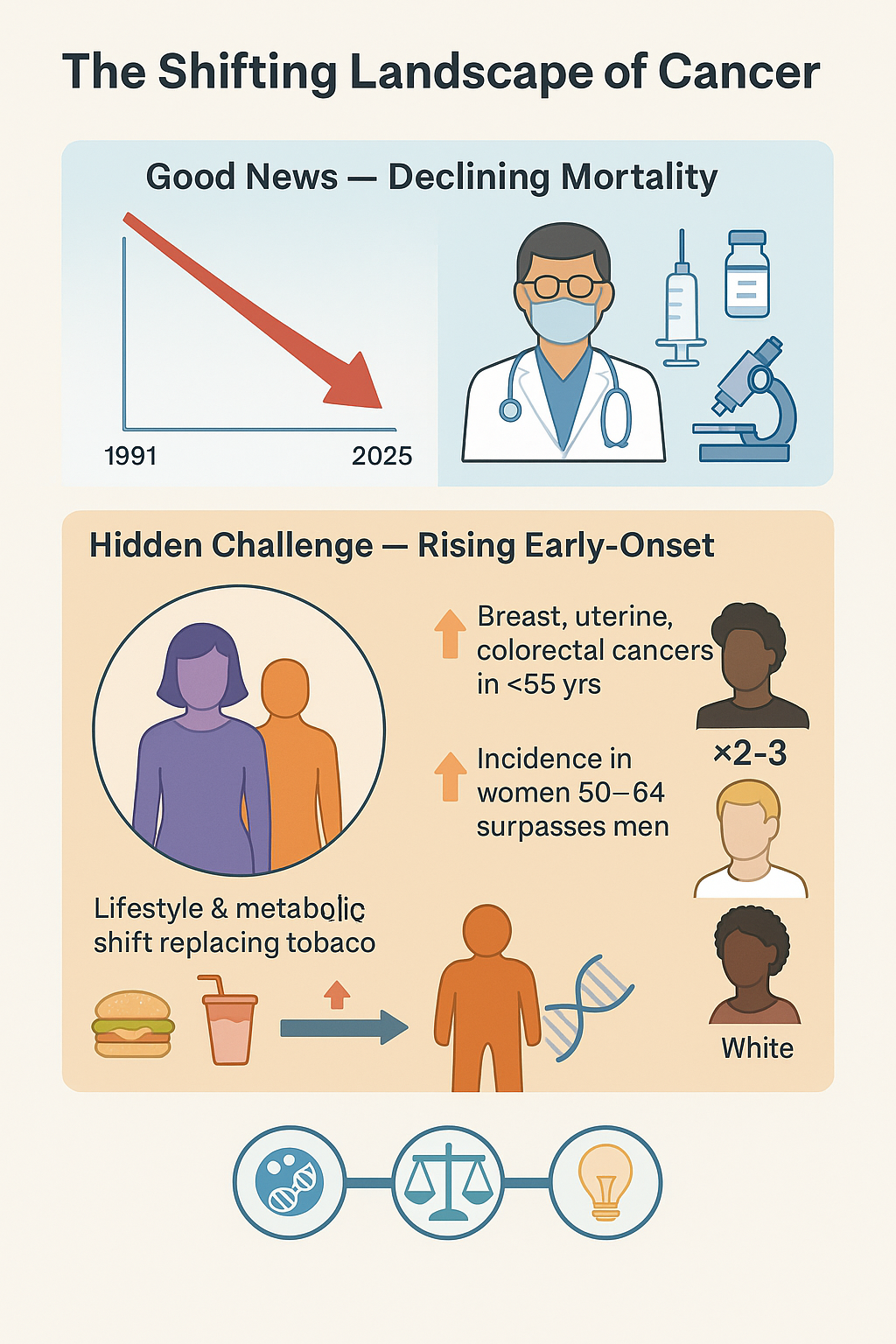
The good news, a 33% drop in U.S. cancer deaths since 1991, masks a troubling demographic shift revealed by the American Cancer Society’s newest statistics. As overall new cases rose from 1.96 million (2023) to 2.04 million (2025), leading to 618,120 expected deaths, the burden is falling unfairly. We’re seeing a rising incidence of breast, uterine corpus, and colorectal cancers in those under 55. For ages 50–64, women now lead men in new diagnoses. Crucially, significant racial gaps persist, with Native American and Black individuals facing two to three times the mortality rate for several cancer types. This evidence points to metabolic and inflammatory environments taking over as the main cancer drivers, moving past tobacco's historical dominance. Our next move must be to fully integrate precision prevention and equitable care access to shift the fight from treatment to early interception.
Keywords: Cancer trends; Early-onset cancer; Prevention.
Introduction
Over the past three decades, the United States has achieved remarkable progress in reducing cancer mortality. From 1991 to 2022, the age-standardized death rate dropped by roughly 33%, translating to nearly 4.5 million deaths averted [1]. In 2025, approximately 2,041,910 new cancer cases and 618,120 deaths are projected, continuing a long-term downward trend in overall mortality [1]. This success story, however, conceals a more complex picture. The latest CA: A Cancer Journal for Clinicians series [1–3] illustrates that the epidemiologic burden of cancer is undergoing a quiet transformation: incidence rates are rising in younger and middle-aged adults, particularly women, even as older populations benefit from better screening, immunization, and targeted therapies. The decline in mortality now coexists with new patterns of inequity and emergent etiologies, signaling that the “war on cancer” has entered a new phase.
Historically, men had far higher cancer rates than women, with a male-to-female incidence ratio of 1.6 in 1992. Yet by 2021, this ratio had narrowed to 1.1, and among individuals aged 50–64, women now surpass men in overall cancer incidence (832.5 vs. 830.6 per 100,000) [1]. Even more striking, women under 50 show an 82% higher incidence rate than their male counterparts (141.1 vs. 77.4 per 100,000), a dramatic increase from the 51% gap observed in 2002 [1]. This reversal is driven by multiple site-specific increases. Breast cancer remains the dominant malignancy in women, with 316,950 new cases expected in 2025, accounting for nearly one-third of female diagnoses [1]. Uterine corpus cancer, once relatively rare, is now among the fastest rising cancers, increasing by 0.6–1% annually since 2015 [2]. Even lung cancer, traditionally male-dominant, has flipped direction: incidence in women under 65 surpassed men for the first time in 2021 (15.7 vs. 15.4 per 100,000) [1]. In the developed world, lifestyle is dethroning tobacco as the key driver of cancer. Obesity, diabetes, and physical inactivity are becoming the dominant, preventable risks. The rise in obesity is particularly concerning; it wreaks havoc on our metabolism, immune system, and hormones, directly driving up rates of endometrial, breast, and colorectal cancers. The central challenge for cancer prevention now is no longer just quitting smoking; it's controlling our metabolism and ensuring equitable health for all.
Perhaps the most alarming trend is the steady rise of early-onset cancers, diagnoses in adults younger than 50 years. Colorectal cancer, once the domain of the elderly, is now the leading cause of cancer death in men under 50 and second in women [2]. Incidence in this group increased 1–2% annually during 2015–2019, even as overall rates fell in older adults. The etiology remains multifactorial: Westernized diets, gut microbiome dysbiosis, antibiotic overuse, and early-life exposures have all been implicated. The implications are profound. A 2025 modeling analysis cited by Siegel et al. estimated that 4,000–7,000 excess colorectal cancer deaths may occur by 2040, depending on how rapidly screening recovers from pandemic disruptions [1]. This “younger shift” in cancer biology calls for a re-examination of screening paradigms. Lowering the starting age for colorectal screening to 45 has been a critical step, yet evidence suggests that even this may not fully capture high-risk populations, especially in underrepresented ethnic groups where screening uptake remains low. A precision-prevention approach, integrating genomic risk scores and lifestyle biomarkers, may soon become essential.
Despite epidemiologic progress, racial disparities remain stark and largely unchanged. The 2025 report highlights that Native American populations experience cancer mortality rates 2–3 times higher than White populations for kidney, liver, stomach, and cervical cancers [1]. Similarly, Black Americans continue to face two-fold higher mortality for prostate, stomach, and uterine corpus cancers. Such inequities are not solely biological, they reflect the cumulative effect of structural determinants: healthcare access, screening availability, and socioeconomic deprivation. For example, while mortality from cervical cancer has plummeted by 65% among vaccinated young women [3], unvaccinated and rural groups remain vulnerable. As the benefits of precision medicine expand, these disparities risk becoming even more entrenched unless prevention, screening, and treatment resources are equitably distributed.
Between 1995 and 2021, the proportion of cancer cases in adults aged ≥65 declined from 61% to 59%, whereas cases in the 50–64 age group rose from 25% to 29% [1]. This demographic shift parallels the “post-war cohort effect,” in which individuals born after 1950 experienced greater lifetime exposure to processed foods, environmental toxins, and sedentary lifestyles. The transition of cancer burden to the middle-aged demographic carries enormous implications for workforce productivity and healthcare cost. Unlike elderly patients, middle-aged individuals are more likely to live long enough to face secondary malignancies and therapy-induced chronic conditions. The need for longitudinal survivorship infrastructure, including cardiovascular monitoring, metabolic management, and psychosocial care, will only intensify.
We used to rely on the American Cancer Society's long-term tracking as the definitive measure, but the 2025 data is a wake-up call: focusing only on lower mortality isn't cutting it. The problem has shifted: incidence rates are climbing right where the impact will be hardest felt, among young people, women, and minority populations. True progress now demands a three-pronged approach: preventing more cancers, closing those stubborn racial gaps, and managing the ongoing health and financial fallout for survivors. Moving forward, cancer control hinges on weaving prevention, genomics, and health equity into a single policy strategy that respects the social and environmental context as much as the molecular one.
Cancer mortality in the U.S. continues to decline, a testament to decades of public health, screening, and therapeutic advances. Yet the battlefront is shifting. Rising incidence in younger and female populations, persistent racial disparities, and the growing influence of metabolic and lifestyle factors all demand a paradigm shift, from cure to early interception and equitable prevention. As Siegel et al. remind us, “continued progress will require investment in cancer prevention and access to equitable treatment, especially for Native American and Black individuals” [1]. The next decade will determine whether we can turn these insights into structural change, or whether success in mortality will mask a new generation of preventable cancers.
Abbreviations
Not Applicable.
Declarations
Author Contributions
Writing: Hengrui Liu; Editing: Ilayda Karsidag.
Acknowledgments
We thank Weifen Chen, Zongxiong Liu, Yaqi Yang, and Bryan Liu for their support.
Funding Information
None.
Ethics Approval and Consent to Participate
Not Applicable.
Competing Interests
The authors declare that the paper was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Data Availability
Not Applicable.
References
 Figures
Figures References
References Peer
Peer Information
InformationPeer-review Terminology
Identity transparency: Single anonymized
Reviewer interacts with: Editor
Details
This is an open access article under the terms of the Creative Commons Attribution License(http://creativecommons.org/licenses/by/4.0/), which permits use, distribution and reproduction in any medium, provided the original work is properly cited.
Publication History
Received 2025-11-07
Accepted 2025-11-11
Published 2025-12-01