


Abstract
Background:Malignant skin melanoma (MSM) and non-melanoma skin cancer (NMSC) have imposed a significant health and economic
burden worldwide. We aim to explore the disease burden and trends of MSM and NMSC, so as to provide references for the prevention
and control of MSM and NMSC.
Methods:Data were derived from the Global Burden of Diseases (GBD) database, covering deaths, disability-adjusted life years
(DALYs), incidence, and prevalence. Joinpoint regression, inequality analysis, decomposition analysis and age-period-cohort (APC)
analysis identified trends and revealed the causes of burden changes from 1990 to 2021. Nordpred package in R projected the future
trends of MSM and NMSC from 2022 to 2044.
Results:From 1990 to 2021, global trends showed an increase in the number of deaths, DALYs, incidence, and prevalence for
MSM, squamous cell carcinoma (SCC), and basal cell carcinoma (BCC). The disease burden was highest in high Socio-Demographic Index
(SDI) region, predominantly concentrated in New Zealand, Australia, and the United States. Among the three skin cancer types, SCC
experienced the most substantial increases in age-standardized incidence (AAPC = 1.62 [95% CI: 1.51 to 1.73]) and prevalence (AAPC =
1.90 [95% CI: 1.78 to 2.02]). The main drivers of DALYs changes were identified as population aging and growth. In the future, the
deaths, DALYs, incidence and prevalence cases of MSM and NMSC will continue to increase.
Conclusion:The disease burden associated with MSM and NMSC remains significant. Primary prevention for newborns and the
elderly should be given top priority. During the prevention of skin cancer, special attention should be paid to SCC. Global medical
resources should be appropriately tilted towards skin cancer.
Keywords:Trend; Inequality; Global burden of disease; Melanoma; Non-melanoma skin cancer.
Introduction
Skin cancer primarily includes malignant skin melanoma (MSM) and non-melanoma skin cancer (NMSC), the latter mainly comprising squamous cell carcinoma (SCC) and basal cell carcinoma (BCC)[1]. MSM originates from melanocytes, which function to produce melanin, thereby protecting the skin against ultraviolet radiation[2]. SCC mainly derives from epidermal keratinocytes[3], while BCC originates from basal cells of the skin[4]. Once these cells become cancerous, the body may have pain and itching symptoms, and the psychology may produce anxiety and fear[5–7]. If skin cancer is not detected and treated early, it may metastasize and become life-threatening[8, 9]. MSM and NMSC represent a significant public health challenge, imposing substantial burdens on healthcare systems worldwide[10]. Australia, New Zealand and the United States have the highest health system costs due to skin cancer[11]. In the United States, the overall estimated annual cost of skin cancer treatment was $8.9 billion between 2016 and 2018[12]. With changing lifestyles and a growing elderly population, skin cancer is becoming an escalating threat across the globe[13]. Therefore, MSM and NMSC should be recognized as critical public health priorities.
Currently, studies have analyzed the burden of MSM and NMSC[14–18]. A study analyzed the burden of MSM and NMSC in the United States from 1990 to 2019[14]. Two studies used the Global Burden of Diseases database (GBD) 2019 and Global Cancer 2022 (GLOBOCAN) databases respectively[15, 16]. The GLOBOCAN 2022 database lacked DALYs indicators and had no data on the major subtypes of NMSC. The remaining studies either only focused on the elderly population or had incomplete indicators[17, 18]. As a result, there is currently no latest and comprehensive global burden evaluation of MSM and NMSC.
We utilized the latest GBD database of 2021 to depict the disease burden of MSM, SCC and BCC. Temporal trends of the three types of skin cancer were analyzed from multiple dimensions. Decomposition analysis was employed to identify the factors contributing to disability-adjusted life years (DALYs). Socioeconomic health inequalities were compared, and future trends in disease burden were projected. Understanding the current disease burden and epidemiological trends is essential for the formulation of effective early prevention and control strategies.
Methods
Study Design and Population
The GBD 2021 database includes data on 371 diseases and injuries across multiple regions and countries. The study retrieved the estimates along with 95% uncertainty intervals (UI) for deaths, DALYs, incidence, and prevalence for MSM and NMSC. As deaths data for BCC were unavailable in the GBD 2021 dataset, analyses of this indicator were excluded. The GBD database does not include deaths data for BCC, primarily due to its extremely low fatality rate and structural limitations in the global data collection system. The Socio-Demographic Index (SDI) measures the development of a country or region by assessing income levels, education levels and health status[19].
Statistical Analysis
To comprehensively understand the burden of MSM, SCC and BCC, we conducted a descriptive analysis. The number and age-standardized rates (ASR) of global deaths, DALYs, incidence and prevalence were visually displayed[20, 21]. We compared the burden of MSM, SCC, and BCC in 2021. We utilized Joinpoint regression to investigate the change trend of three types of skin cancer[22, 23]. The age-period-cohort model was employed to analyze the underlying trends in incidence among different ages, periods, and birth cohorts[24, 25]. We conducted decomposition analysis on the potential factors driving the DALYs of MSM, SCC and BCC[26]. The distribution of health inequalities related to MSM, SCC, BCC burden across countries was evaluated[27]. To forecast the future burden of MSM, SCC, and BCC for the next 23 years, the Norpred package in R was used[28, 29]. These methods were described in detail in Supplementary Methods.
Results
Descriptive analysis of MSM and NMSC in 2021
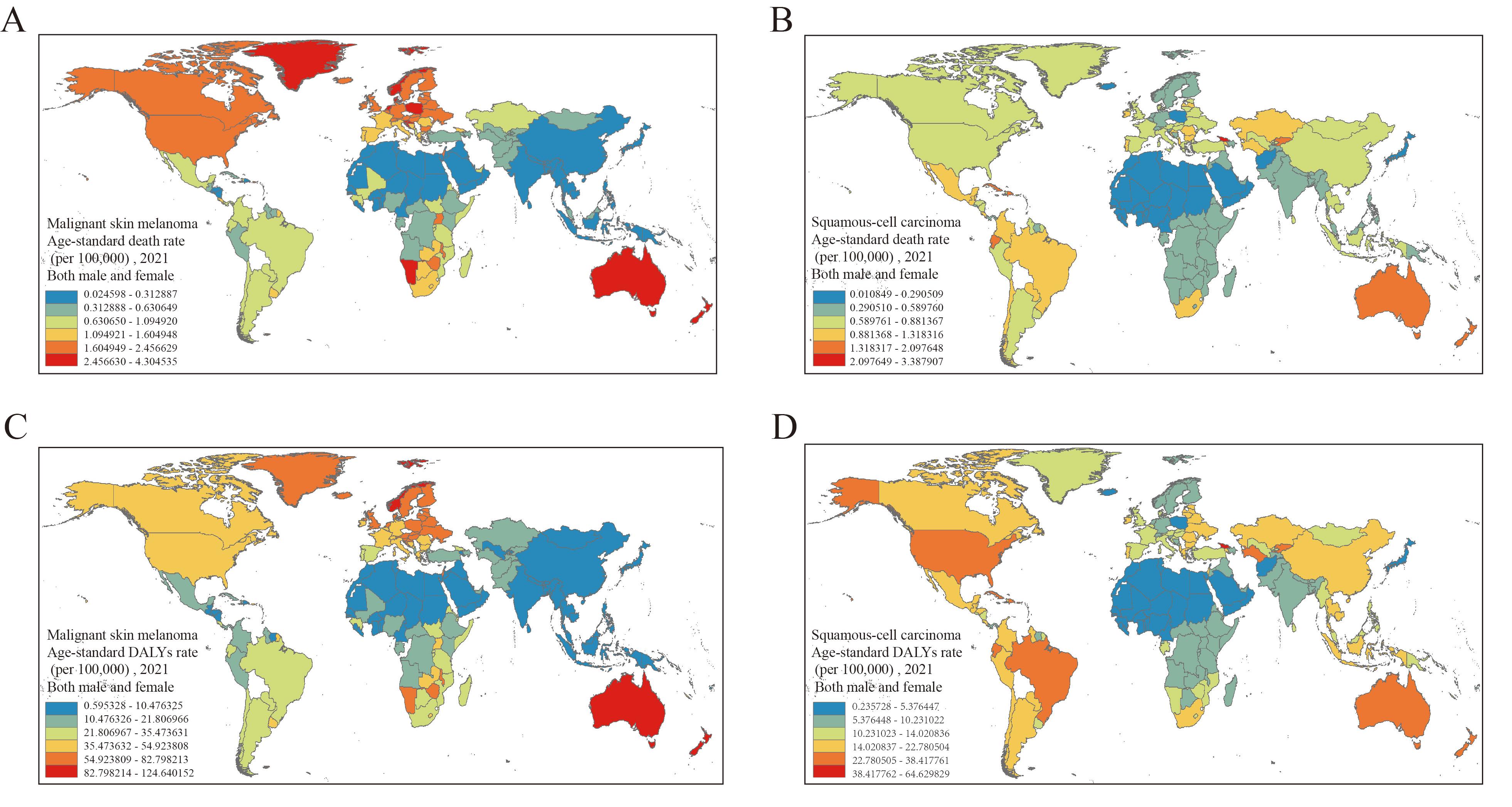
From 1990 to 2021, the global burden of MSM, SCC, and BCC demonstrated a significant upward trend in the numbers of deaths, DALYs, incidence and prevalence (Figure S1). In 2021, MSM exhibited the highest age-standardized death rate (ASDR) (0.73 [95% UI, 0.65, 0.79]) and age-standardized DALYs rate (ASDALYs) (19.63 [95% UI, 17.25, 21.50]). BCC had the highest age-standardized incidence rate (ASIR) (51.71 [95% UI, 45.70, 57.58]), while SCC presented the highest age-standardized prevalence rate (ASPR) (26.85 [95% UI, 22.77, 31.77]) (Tables S1-S3). The high SDI region had the highest ASR of deaths, DALYs, incidence, and prevalence. (Figure S3). Among the 21 GBD regions, Western Europe exhibited the highest burden for MSM in numbers of deaths, DALYs, incidence and prevalence (Table S4). High-income North America had the highest incidence and prevalence of BCC (Table S5). East Asia had the highest numbers of deaths, DALYs and prevalence of SCC (Table S6). The ASRs for deaths, DALYs, incidence, and prevalence of the three types of skin cancer varied significantly between countries around the world. Specifically, New Zealand had the highest ASDR, ASDALYs, ASIR and ASPR for MSM, while the United States of America exhibited the highest ASIR and ASPR for SCC and BCC (Figure 1, Figure S2). In addition, the disease burden of skin cancer was mainly concentrated in older adults and males (Figure S4).
Figure 1. Age-standardized rates of deaths and DALYs attributed to MSM and SCC in 2021. (A, B) death. (C, D) DALYs. DALYs = disability-adjusted life years. MSM = malignant skin melanoma. SCC = squamous cell carcinoma.
Trends in MSM and NMSC using joinpoint analysis
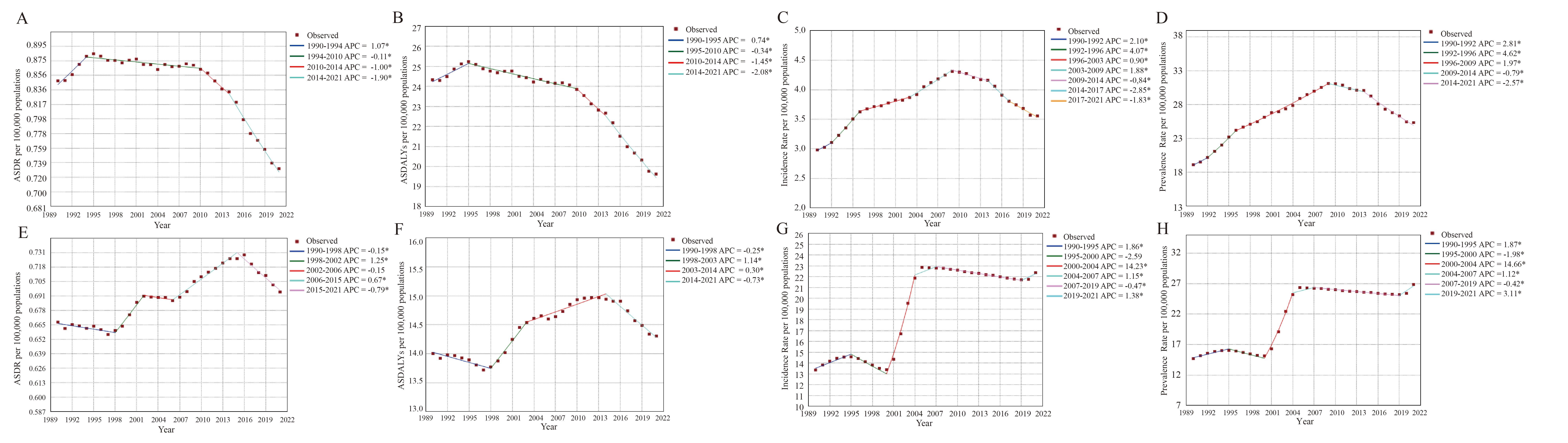
From 1990 to 2021, the trend in ASDR (AAPC = -0.48 [95% CI: -0.37 to -0.59]) and ASDALYs (AAPC = -0.71 [95% CI: -0.60 to -0.82]) for MSM showed a decline (Table S7). Conversely, the ASIR and ASPR for MSM increased over time with AAPC values of 0.56 (95% CI: 0.33 to 0.79) and 0.87 (95% CI: 0.68 to 1.06) (Table S7). For SCC, the AAPC values for ASDR, ASDALYs, ASIR and ASPR were 0.14 (95% CI: 0.06 to 0.22), 0.06 (95% CI: 0.03 to 0.08), 1.62 (95% CI: 1.51 to 1.73) and 1.90 (95% CI: 1.78 to 2.02), respectively (Table S7). The ASDR and ASDALYs of SCC showed a downward trend since 2015. During the period from 2000 to 2004, ASIR and ASPR of SCC had the fastest growth rates, where the annual percentage change values were 14.23 (95% CI: 13.75 to 14.71) and 14.66 (95% CI: 14.16 to 15.16), respectively. From 2007 to 2021, the ASIR and ASPR of SCC remained at a relatively high level (Figure 2). The ASIR and ASPR of BCC were similar to that of SCC (Figure S5).
Figure 2. Global temporal trends in ASDR, ASDALYs, ASIR, and ASPR attributed to MSM and SCC based on the joinpoint regression analysis (1990-2021). (A-D) MSM. (E-H) SCC. (A, E) ASDR. (B, F) ASDALYs. (C, G) ASIR. (D, H) ASPR. ASDR = Age-standardized death rate. ASDALYs = Age-standardized DALYs rate. ASIR = Age-standardized incidence rate. ASPR = Age-standardized prevalence rate. MSM = malignant skin melanoma. SCC = squamous cell carcinoma. *Indicates that the annual percent change is significantly different from zero at the alpha = 0.05 level.
Age-period-cohort analysis of incidence in MSM and NMSC
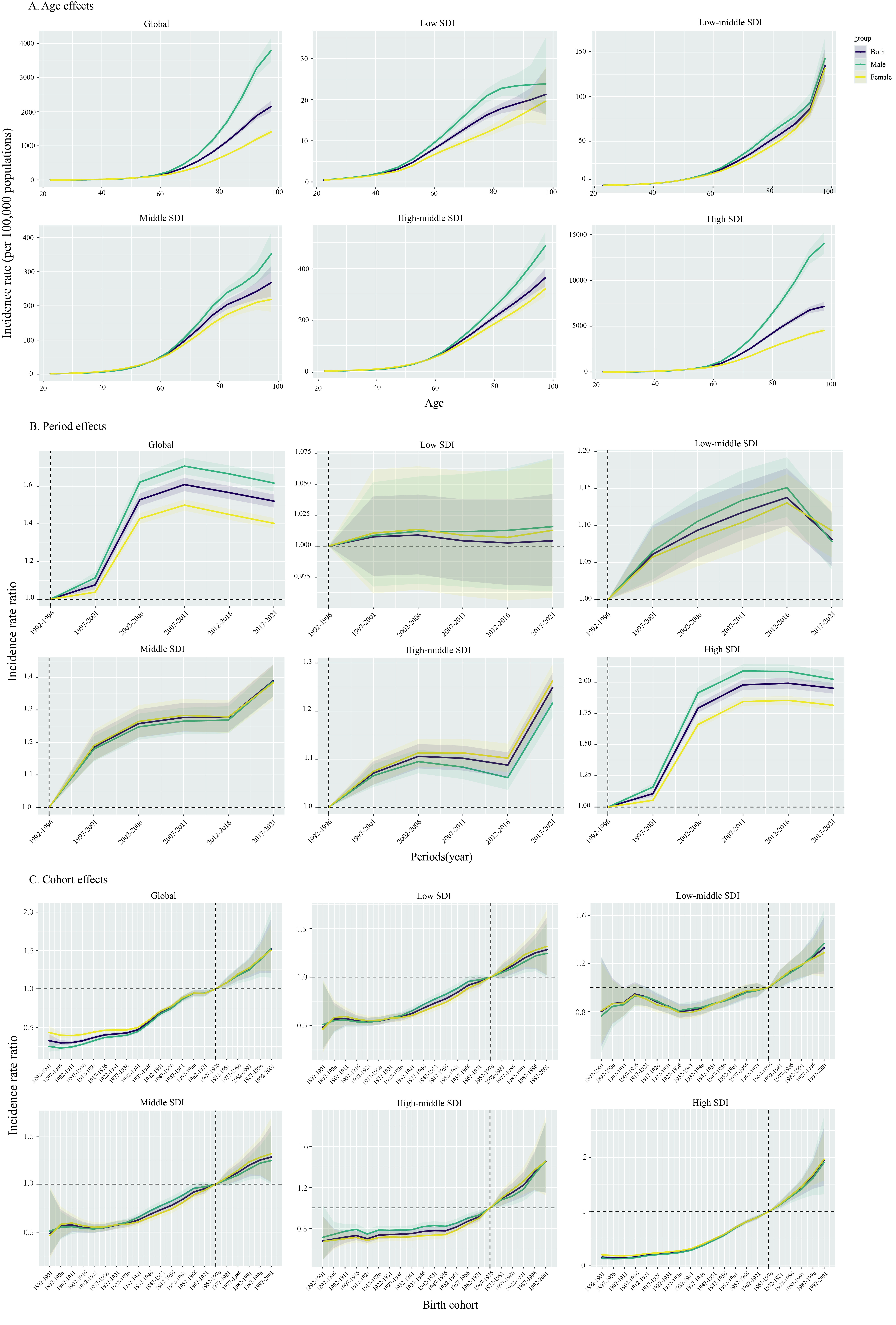
The age effect curve shows that the risk of skin cancer increases with aging (Figure 3, Figure S6-S7). Among the SDI regions, high SDI countries consistently demonstrated the highest incidence across all age groups, with male showing a higher incidence than female. Regarding period effects, the overall trend of SCC and BCC presented an upward tendency. Globally, the upward trends were more prominent among male than female. For MSM and SCC, the incidence increased globally between 1992 and 2011, but decreased between 2011 and 2021 (Figure S6-S7). For MSM, the global cohort effects peaked in the 1942 to 1951 birth cohort (Figure S6). Among post-1952 birth cohorts, an improvement in the burden of MSM was only observed in high SDI regions. A significant gender-based difference in cohort effects between male and female was noted in high SDI regions for individuals born around 1945. For SCC and BCC, the birth cohort effects were on the rise overall, globally and five SDI regions, reaching a maximum in the 1992 to 2001 birth cohort with no significant difference between male and female (Figure 3).
Figure 3. The age–period–cohort analysis of BCC in global and five SDI regions. (A) Longitudinal age curve. (B) Period rate ratio. (C) Cohort rate ratio. BCC = basal cell carcinoma. SDI = socio-demographic index.
Decomposition analysis regarding DALYs in MSM and NMSC
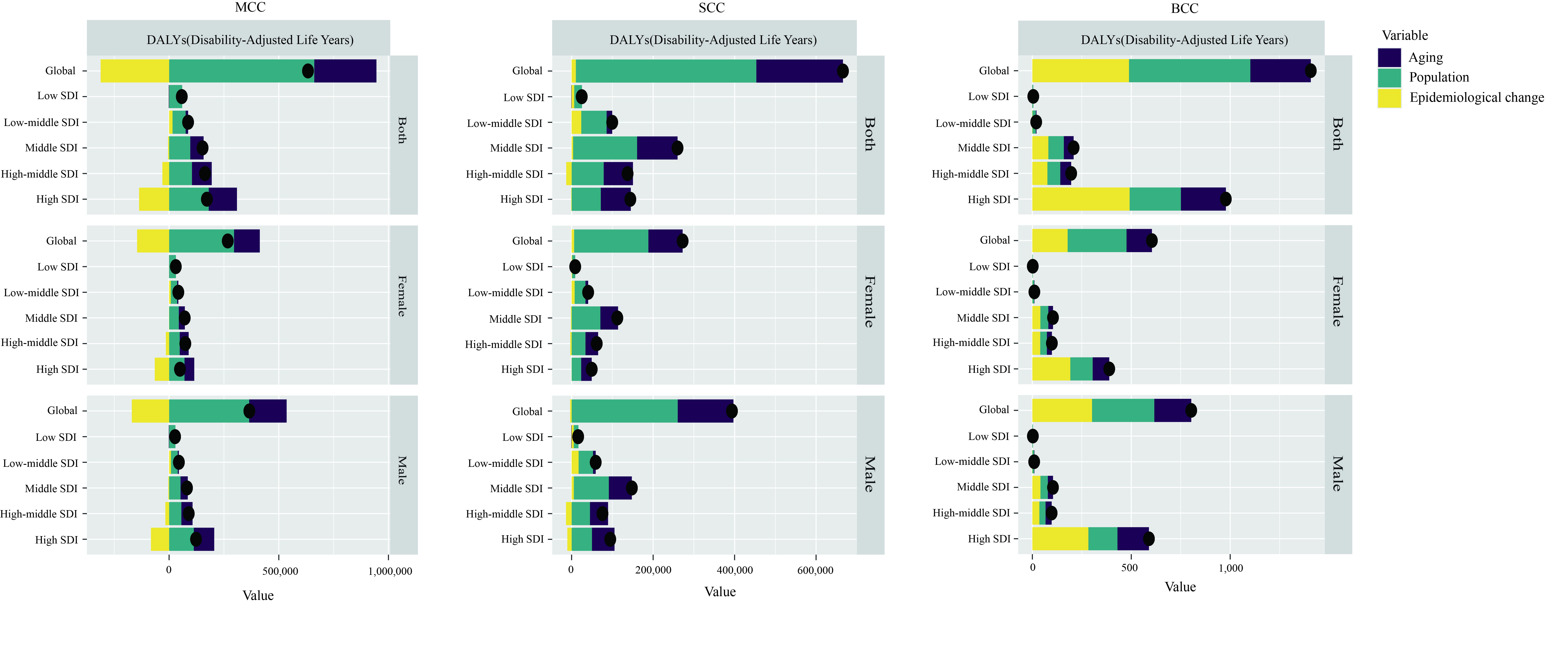
From 1990 to 2021, there was a significant increase in DALYs for three types of skin cancer globally, with the largest increase for MSM and BCC in high SDI regions and the largest increase for SCC in middle SDI regions (Figure 4). For the three types of skin cancer, the overall increase was larger in males than females. For MSM, the contribution of aging, population growth, and epidemiological changes to the global increase in DALYs was 36.23%, 112.88%, and -49.12%, respectively (Table S8). Population growth emerged as the most influential factor driving DALYs increases across all SDI regions, while epidemiological changes had a negative impact, particularly in high SDI regions. For SCC, aging, population growth, and epidemiological changes contributed 31.95%, 66.51%, and 1.54% to the global increase in DALYs, respectively (Table S8). In high and high-middle SDI regions, aging and population factors had nearly equal impacts on the rise in DALYs, while in other SDI regions, population growth played the dominant role. For BCC, aging, population growth and epidemiological changes contributed 21.72%, 43.58%, and 34.70% to the global increase in ASDALYs, respectively (Table S8). Notably, epidemiological changes had the largest impact on DALYs in high SDI regions, whereas population growth emerged as a critical determinant of DALYs in low SDI regions.
Figure 4. Changes in DALYs of MSM, SCC, BCC according to aging, population growth and epidemiological change from 1990 to 2021 at global level by SDI regions and sexes. The black dot denotes the overall value of the change resulting from all three components. For each component, the magnitude of a positive value suggests a corresponding increase in DALYs attributed to the component; the magnitude of a negative value suggests a corresponding decrease in DALYs attributed to the component. DALYs = disability-adjusted life years. MSM = malignant skin melanoma. SCC = squamous cell carcinoma. BCC = basal cell carcinoma. SDI = socio-demographic index.
Cross-country inequality analysis regarding incidence in MSM and NMSC
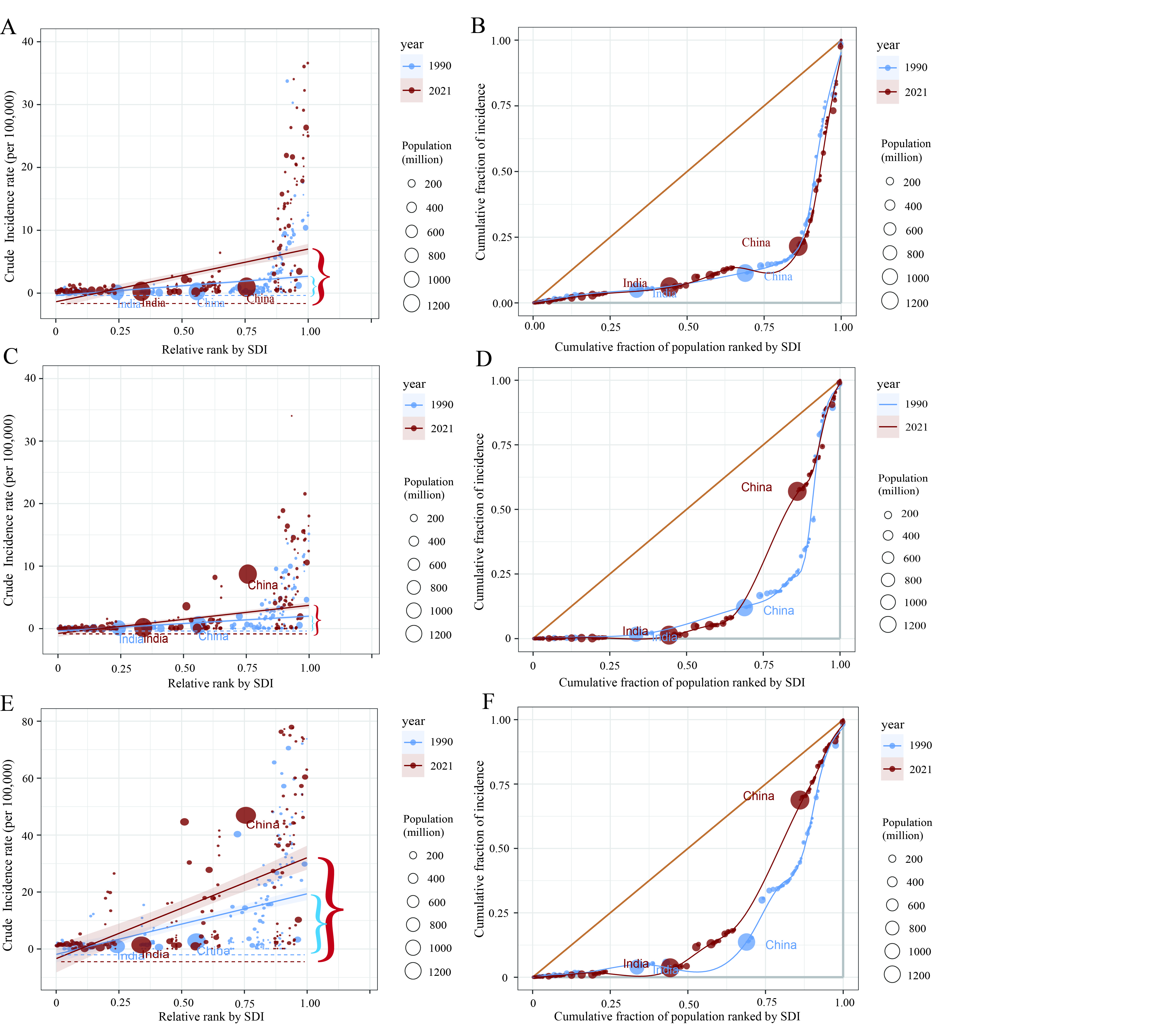
The absolute inequality in the burden of the three types of skin cancer associated with SDI increased over time. A higher proportion of incidence was observed in countries characterized by advanced socio-demographic development (Figure 5). In 1990, the slope index of incidence for MSM stood at 3.06 (95 %UI 2.34, 3.78) per 100,000 people, and it increased to 9.53 (95 %UI 7.36, 11.70) in 2021, showing that the wealthiest country had an incidence rate approximately 9.53 per 100,000 individuals higher than the poorest country (Table S9). The slope index of SCC and BCC showed a similar growth trend to that of MSM, but the increase in BCC was more pronounced.
Figure 5. Health inequality regression curves and concentration curves for the incidence of MSM, SCC and BCC worldwide, 1990 and 2021. (A, B) MSM. (C, D) SCC. (E, F) BCC. DALYs = disability-adjusted life years. MSM = malignant skin melanoma. SCC = squamous cell carcinoma. BCC = basal cell carcinoma. SDI = socio-demographic index.
Predictive analysis in MSM and NMSC until 2044
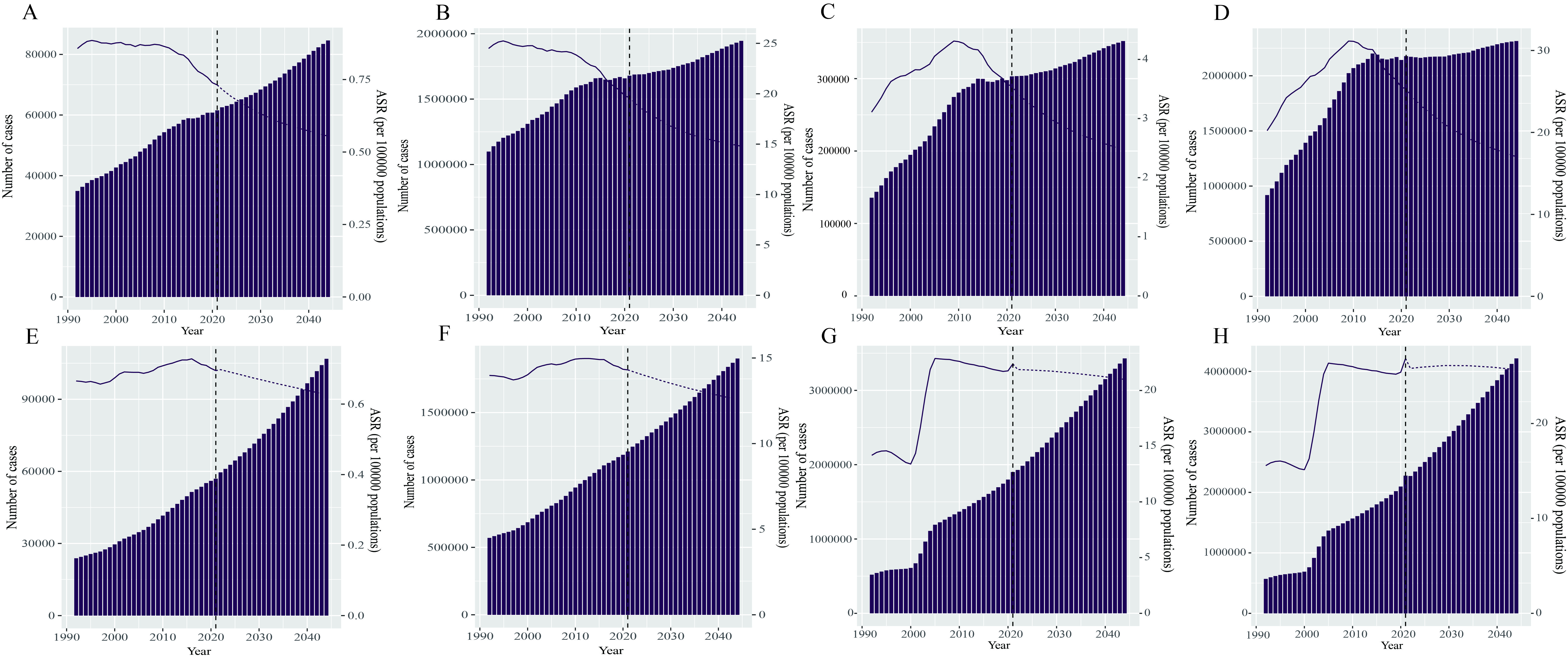
From 2022 to 2044, the incidence numbers for MSM, SCC and BCC were predicted to increase from 303,431, 1,928,413, and 4,376,687 to 351,863, 3,429,869 and 7,362,321 (Table S10), with increase of approximately 15.96%, 77.86% and 68.22%, respectively. In recent years, the gap of number of deaths between SCC and MSM has been progressively narrowing. It is predicted that by 2025, the number of deaths attributable to SCC will surpass that of MSM. Over the next 23 years, the numbers of deaths and DALYs, and the prevalence for the three types of skin cancer will all increase (Figure 6, Figure S8). By 2044, the ASR for deaths, DALYs, incidence, and prevalence of MSM will decline to 0.55 per 100,000 people, 14.79, 2.47, and 17.03 respectively (Table S11). The changing trends of SCC and BCC were similar to those of MSM, but the declines were relatively slight (Figure 6, Figure S8).
Figure 6. Trends in the number and age-standardized rates of deaths, DALYs, incidence, and prevalence attributed to MSM and SCC globally in the next 23 years (2022 - 2044). (A - D) MSM. (E - H) SCC. (A, E) deaths. (B, F) DALYs. (C, G) incidence. (D, H) prevalence. DALYs = disability-adjusted life years. MSM = malignant skin melanoma. SCC = squamous cell carcinoma. ASR = age-standardized rate.
Discussion
The study utilized the latest data to analyze the global trends of deaths, DALYs, incidence, and prevalence for the three types of skin cancer from 1990 to 2021. Globally, the numbers of deaths, DALYs, incidence and prevalence for the three types of skin cancer showed upward trends. The disease burden in Western Europe and High-income North America was relatively more severe. Males exhibited higher burden of the three types of skin cancer compared to females. Compared to previous similar studies, there are many new findings. (1) In 2021, MSM exhibited the highest ASDR and ASDALYs. BCC had the highest ASIR, and SCC had the highest ASPR. (2) Among the three types of skin cancer, SCC displayed the most pronounced upward trends in ASIR and ASPR from 2000 to 2004. (3) Age and birth cohort showed an upward trend of the three skin cancers with time. (4) Decomposition analysis showed that aging and population growth were the primary contributors to the increase of DALYs. (5) The incidence rate was higher in high SDI countries, and the inequality intensified over time. (6) While the ASR for deaths, DALYs, incidence, and prevalence for the three types of skin cancer was expected to decline until 2044, the absolute number for these metrics was projected to rise.
In 2021, MSM exhibited the highest ASDR and ASDALYs. BCC had the highest ASIR, while SCC showed the highest ASPR. Although MSM accounted for only 3% of all skin cancers, its mortality accounts for 65% of all skin cancers[30]. MSM had the highest ASDR among the three types of skin cancer because it is a highly aggressive skin tumor. The global health system should establish a special scientific research fund for MSM, encourage global scientific research institutions to collaborate with medical institutions, to deeply explore the pathogenesis and the patterns of invasion and metastasis, and accelerate the research and development of innovative treatment technologies. The incidence of BCC and SCC was higher than that of MSM. This result indicated that in the formulation of relevant health strategies, the prevention of NMSC should be placed in the primary position.
Significant variations in the burden of the three types of skin cancer were observed across different countries and regions. While East Asia accounts for the highest absolute numbers of SCC deaths and DALYs globally, high-SDI regions exhibit the highest standardized rates of these outcomes. This may be related to the following reasons. First, the huge population base in East Asia directly increases the absolute number of SCC deaths and DALYs. Second, East Asia is experiencing rapid aging, with a large absolute number of elderly people, further magnifying the overall scale of SCC deaths and DALYs[31]. Third, the core purpose of age standardization is to eliminate the differences in age structure between different regions. The higher standardized rate in high SDI regions may be related to risk exposure factors in this region, such as longer ultraviolet (UV) exposure time and higher skin cancer screening rates[32]. In view of the differences of skin cancer in different regions, a dynamic resource allocation mechanism for skin cancer should be established. At the same time, efforts should be made to promote the sharing of medical resources, and narrow the gap in the diagnosis and treatment levels of skin cancer between regions through means such as telemedicine and expert rounds.
In 2021, gender-stratified analysis revealed that males bore a higher disease burden than females across three skin cancer types. It is important to clarify that the "male" and "female" categories referenced in this study align with the biological sex classifications defined by the GBD Study, reflecting inherent biological traits rather than social gender identities or gender roles. The observed sex differences in SCC burden are not attributable to essentialist notions of inherent vulnerability or resistance to the disease, but instead are mediated by key behavioral and occupational factors[33, 34]. A study revealed that the ASDR of MSM among males was 30% higher than that among females[35]. This difference could be explained by the following perspectives. In some outdoor jobs, males constitute the majority of practitioners[36, 37]. Differences in sunscreen use and attitudes to asymptomatic illness may explain the difference[38]. Therefore, all countries should make full use of this gender difference and formulate targeted prevention and intervention strategies. Regulations should be established to limit the working hours of outdoor workers in policies and build sun-protection areas for them.
Joinpoint regression method is a highly effective tool in data analysis and trend research. It divides the overall trend precisely into multiple distinct phases. We found that among the three types of skin cancer, the increasing trends in ASIR and ASPR of SCC and BCC were the most significant. In addition, the most rapid increase occurred between 2000 and 2004. The following reasons may account for this result. Skin detection technology has improved. With the development of optical technology, dermoscopy technology has gradually emerged[39]. Entering the 21st century, the integration of computer and imaging technology further facilitated the development of more efficient detection methods. Additionally, the increasing aging of the population has contributed to the rising burden of skin cancer, especially for SCC and BCC[40]. Since 2010, the ASIR and ASPR of the three types of skin cancer have shown a downward trend. This can be attributed to increased public awareness of sun protection. Primary prevention is the most effective measure for preventing skin cancer[41]. Therefore, it is necessary to formulate a national health education plan for skin cancer and carry out publicity of skin cancer prevention knowledge. In Australia and the United States of America, preventive initiatives including sun protection education and increased use of sunscreen have been implemented[42].
We explored the trends of skin cancer across three temporal dimensions. The incidence rates of the three types of skin cancer increase with age, and the increasing speed became even faster starting from the age range of 50 to 60. With increasing age, the self-repair ability of the skin declines, and it is difficult to repair DNA damage in a timely manner after being damaged by carcinogenic factors[43, 44]. The relative incidence risk trended upward, suggesting that later-born individuals faced higher risks. Consequently, effective preventive and management measures need to be taken for people in this age group. For the elderly and newly born population, regular skin examination and screening programs should be strengthened. For these two groups, it is particularly important to promote the use of safe protective supplies.
Cross-country inequality analysis revealed that the gap in health inequality between low and high SDI regions is expanding. This growing inequality may be the result of economic uncertainty and inadequate public health policies. This indicated that a transnational skin cancer research and monitoring network should be established, where countries could share data, including incidence rates, risk factors, treatment strategies, and prognostic outcomes. Such a network would facilitate a deeper understanding of the evolving trends in inequality and provide a strong foundation for future intervention measures and optimal resource allocation.
While the ASDR, ASDALYs, ASIR, and ASPR for MSM and NMSC were forecasted to decline, the absolute numbers for these four indicators were forecasted to rise. This distinction is not only essential for the accurate interpretation of epidemiological indicators but also critical for effective public health messaging[45, 46]. The decline in ASIR reflects the success of recent primary prevention efforts for SCC, including widespread sun protection education, improved occupational UV exposure controls, and enhanced early detection initiatives—demonstrating that disease risk at the population level has been substantially reduced. Nevertheless, the projected rise in absolute case numbers should not be interpreted as a failure of these interventions; instead, it is primarily driven by demographic dynamics such as population growth and aging, which increase the total number of susceptible individuals. The rise in numbers was attributable to alterations in population structures, lifestyle and living environments. Decomposition analysis showed that population growth and aging were the main causes of the increase in global DALYs for skin cancer. The process of global population ageing is accelerating continuously. The continuous increase in the global population and the acceleration of the aging process have formed the basic framework for the increase in the disease burden[47]. In addition, the popularity of sun-worshipping culture has led to a significant increase in the time spent on outdoor leisure activities. Therefore, policymakers should seize the opportunity of changes in population structure and lifestyle to improve the healthcare system, consequently enhancing the efficiency and quality of medical services.
Based on the analysis of the regional and population characteristics of the disease burden of SCC, the research results can be translated into the following primary prevention levers, and differentiated strategies should be implemented in combination with the differences in resource endowments and disease drivers between high and low SDI regions. In high SDI regions, (1) Early-life photoprotection: Strengthen structured sun-protection policies and ensure early access to effective photoprotection; (2) Occupational UV exposure: Enforce UV-safety regulations and improve protective measures for outdoor workers; (3) Older-adult screening: Expand routine skin examinations and promote early recognition of lesions; (4) SCC focus: Prioritize surveillance of high-risk groups and streamline diagnostic pathways. In low SDI regions, (1) Early-life photoprotection: Promote low-cost protective behaviors to maintain currently low exposure levels; (2) Occupational UV exposure: Provide basic UV-safety education and simple protective solutions for outdoor laborers; (3) Older-adult screening: Utilize opportunistic screening and enhance lesion recognition in primary care; (4) SCC focus: Improve basic awareness and diagnostic capacity to prevent future burden increases.
Our study had the following limitations. First, regarding the inherent bias of secondary data, although the GBD 2021 data provided support for the integrated analysis of the global burden of skin cancer, its core limitation lies in the heterogeneity of the data sources. Second, the underreporting of skin cancer cases in low-income and middle-income countries is driven by a combination of factors, including limited healthcare access, fragmented or underdeveloped tumor registry systems, and patient-level cognitive barriers. Third, due to the lack of internal data for each country, it is difficult to conduct a detailed analysis of the internal trends within countries.
Conclusions
The disease burden of MSM and NMSC is substantial and is expected to increase in the coming years. The global health inequality in the disease burden of MSM and NMSC persists over time. Globally, there is a need to increase the allocation of medical resources for MSM and NMSC, particularly targeting the elderly population.
Abbreviations
age-standardized rates: ASR; age-standardized death rate: ASDR; age-standardized DALYs rate: ASDALYs; age-standardized incidence rate: ASIR; age-standardized prevalence rate: ASPR; basal cell carcinoma: BCC; disability-adjusted life years: DALYs; Global Burden of Diseases: GBD; Malignant skin melanoma: MSM; Non-melanoma skin cancer: NMSC; squamous cell carcinoma: SCC; Socio-Demographic Index: SDI.
Supplementary Materials
Declarations
Author Contributions
Zhan Li: Writing – review & editing, Writing – original draft. Yuqin Tang: Data curation, Formal analysis. Yuan Chen: Writing – review & editing, Validation. Yuxin Wang:Conceptualization. Yaping Feng:Writing – review & editing. Yue Li:Writing – review & editing. Yingying Yu: Data curation, Formal analysis. Mingyi Zhang:Data curation, Formal analysis. Fang Wang:Validation, Funding acquisition, Data curation.
Acknowledgments
We highly appreciate the work by the GBD 2021 collaborators.
Funding Information
This study was supported by the Natural Science Foundation for the Higher Education Institutions of Anhui Province of China (2022AH051145), the Research Fund of Anhui Institute of translational medicine (2022zhyx-C35).
Ethics Approval and Consent to Participate
Not Applicable.
Competing Interests
The authors declare that they have no existing or potential commercial or financial relationships that could create a conflict of interest at the time of conducting this study
Data Availability
Not Applicable.
References
[7] Venger O, Zhulkevych I, & Mysula Y. (2021). PSYCHOLOGICAL AND PSYCHOPATHOLOGICAL FEATURES OF PATIENTS WITH SKIN CANCER. Georgian Med News, (315), 29-33.
[10] Yusuf N. (2023). Immunomodulation of Skin Cancer. Int J Mol Sci, 24(13).
[44] Moriwaki S, & Takahashi Y. (2008). Photoaging and DNA repair. J Dermatol Sci, 50(3), 169-176.
 Figures
Figures References
References Peer
Peer Information
InformationFigure 1. Age-standardized rates of deaths and DALYs attributed to MSM and SCC in 2021. (A, B) death. (C, D) DALYs. DALYs = disability-adjusted life years. MSM = malignant skin melanoma. SCC = squamous cell carcinoma.
Figure 2. Global temporal trends in ASDR, ASDALYs, ASIR, and ASPR attributed to MSM and SCC based on the joinpoint regression analysis (1990-2021). (A-D) MSM. (E-H) SCC. (A, E) ASDR. (B, F) ASDALYs. (C, G) ASIR. (D, H) ASPR. ASDR = Age-standardized death rate. ASDALYs = Age-standardized DALYs rate. ASIR = Age-standardized incidence rate. ASPR = Age-standardized prevalence rate. MSM = malignant skin melanoma. SCC = squamous cell carcinoma. *Indicates that the annual percent change is significantly different from zero at the alpha = 0.05 level.
Figure 3. The age–period–cohort analysis of BCC in global and five SDI regions. (A) Longitudinal age curve. (B) Period rate ratio. (C) Cohort rate ratio. BCC = basal cell carcinoma. SDI = socio-demographic index.
Figure 4. Changes in DALYs of MSM, SCC, BCC according to aging, population growth and epidemiological change from 1990 to 2021 at global level by SDI regions and sexes. The black dot denotes the overall value of the change resulting from all three components. For each component, the magnitude of a positive value suggests a corresponding increase in DALYs attributed to the component; the magnitude of a negative value suggests a corresponding decrease in DALYs attributed to the component. DALYs = disability-adjusted life years. MSM = malignant skin melanoma. SCC = squamous cell carcinoma. BCC = basal cell carcinoma. SDI = socio-demographic index.
Figure 5. Health inequality regression curves and concentration curves for the incidence of MSM, SCC and BCC worldwide, 1990 and 2021. (A, B) MSM. (C, D) SCC. (E, F) BCC. DALYs = disability-adjusted life years. MSM = malignant skin melanoma. SCC = squamous cell carcinoma. BCC = basal cell carcinoma. SDI = socio-demographic index.
Figure 6. Trends in the number and age-standardized rates of deaths, DALYs, incidence, and prevalence attributed to MSM and SCC globally in the next 23 years (2022 - 2044). (A - D) MSM. (E - H) SCC. (A, E) deaths. (B, F) DALYs. (C, G) incidence. (D, H) prevalence. DALYs = disability-adjusted life years. MSM = malignant skin melanoma. SCC = squamous cell carcinoma. ASR = age-standardized rate.
[7] Venger O, Zhulkevych I, & Mysula Y. (2021). PSYCHOLOGICAL AND PSYCHOPATHOLOGICAL FEATURES OF PATIENTS WITH SKIN CANCER. Georgian Med News, (315), 29-33.
[10] Yusuf N. (2023). Immunomodulation of Skin Cancer. Int J Mol Sci, 24(13).
[44] Moriwaki S, & Takahashi Y. (2008). Photoaging and DNA repair. J Dermatol Sci, 50(3), 169-176.
Peer-review Terminology
Identity transparency: Single anonymized
Reviewer interacts with: Editor
Details
This is an open access article under the terms of the Creative Commons Attribution License(http://creativecommons.org/licenses/by/4.0/), which permits use, distribution and reproduction in any medium, provided the original work is properly cited.
Publication History
Received 2025-09-16
Accepted 2025-12-16
Published 2026-01-04