


Abstract
Background:Esophageal adenocarcinoma (EAC) is a malignant tumor that has been increasing in incidence over the past few decades. Identifying the risk factors associated with EAC is crucial for prevention and early detection strategies.
Methods:This study aimed to investigate the potential risk factors for EAC using a Mendelian randomization (MR) approach. We attained genetic variants associated with 52 exposure factors s from available large-scale genome-wide association studies.
Results:Genetic predisposition to childhood body mass index, forced expiratory volume in 1-second, glomerular filtration rate, telomere length, alcohol consumption, anxiety or depression, smoking, coffee consumption, time spent watching television, basal metabolic rate, body fat percentage, body mass index, hip circumference, obesity class 1, obesity class 2, trunk fat percentage, waist circumference, waist-to-hip ratio, iron, Barrett's esophagus, and gastroesophageal reflux disease were associated with increased risk of EAC. In addition, we demonstrated that age at first birth, age at first sexual intercourse, age at menarche, years of schooling, type 1 diabetes, and fruit intake could suggestively decrease the odds of EAC.
Conclusion:This study represents the inaugural MR investigation to present a comprehensive atlas of risk factors associated with EAC, which will aid in advancing the formulation of efficacious preventive and early detection approaches.
Keywords: Esophageal adenocarcinoma, Mendelian randomization, single-nucleotide polymorphisms, risk factor, early detection
Introduction
Esophageal carcinoma is globally positioned as the eighth most prevalent form of cancer, and ranks as the sixth leading contributor to cancer-related mortality [5] . While esophageal squamous cell carcinoma maintains a significant presence worldwide, the incidence of esophageal adenocarcinoma (EAC) is progressively assuming a dominant role in developed nations [4] . EAC exhibits a markedly favorable prognosis when identified at an early stage, confined to the mucosal and submucosal layers of the esophagus. However, the majority of cases are detected at advanced stages, where outcomes remain poor [7,20] . The 5-year overall survival rate for patients with esophageal adenocarcinoma is less than 20%, a figure comparable to the dismal survival rates observed in malignancies of the liver, lung, and pancreas [7,20] . These statistics underscore the urgent need for the development and implementation of effective screening strategies to facilitate earlier diagnosis and improve patient outcomes.
In efforts to thwart the progression of EAC, the implementation of effective screening strategies is anticipated to assume a pivotal role, consequently presenting a promising avenue for reducing mortality rates in the future. Currently, smoking, gastroesophageal reflux disease, and Barrett esophagus stand recognized as the principal risk factors accountable for EAC development [4] . However, our current comprehension of additional potential risk factors for EAC remains restricted. Moreover, the execution of randomized controlled trials aimed at investigating these risk factors poses considerable challenges, thereby predominantly relying on observational studies to offer valuable insights. It is crucial to recognize the inherent limitations of observational studies, including limited sample sizes and inadequate adjustment for confounding variables, which can potentially compromise the accurate assessment of cancer development. Hence, there arises a pressing necessity for a groundbreaking approach to effectively estimate the causal risk factors associated with EAC. Mendelian randomization (MR) analysis, employing single nucleotide polymorphisms (SNPs) as instrumental variables (IVs), stands as an innovative methodology for elucidating causal inferences between exposures and outcomes [2,11] . Of remarkable significance, this epidemiological approach serves to mitigate the impact of potential confounding factors [2,11] . Against this backdrop, we embarked upon an MR analysis utilizing a vast cohort of European individuals, with the aim of constructing a comprehensive compendium of the risk factors intricately associated with EAC.
Methods
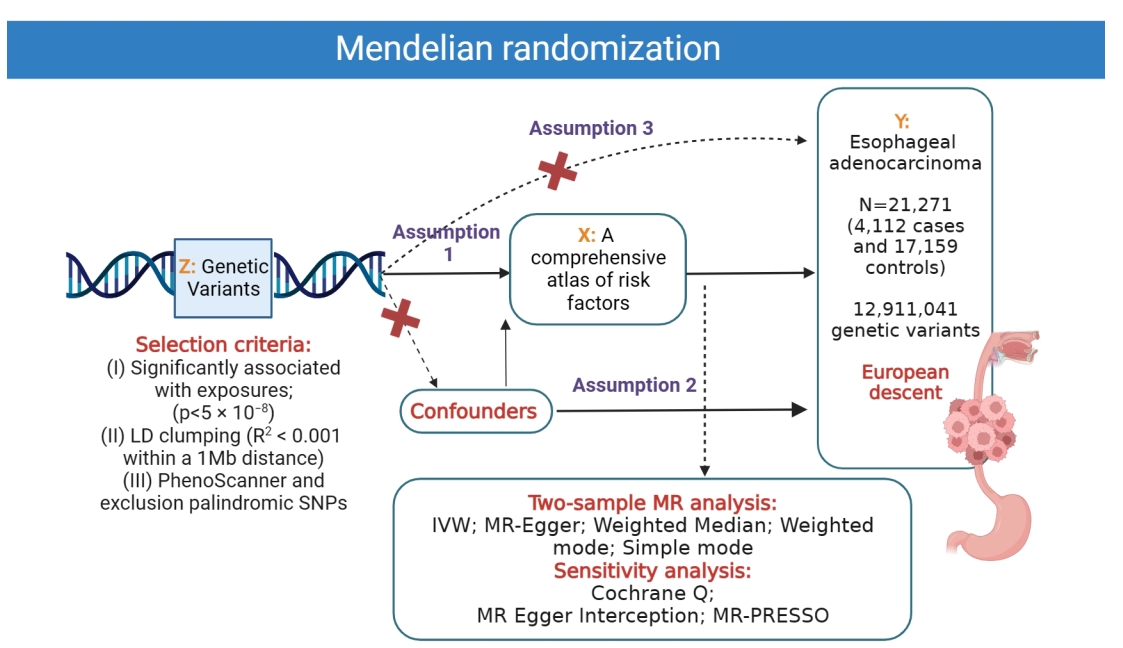
The study examined 52 risk factors associated with EAC using MR analysis and summary-level data from large-scale GWASs (Supplementary Table S1, Figure 1). SNPs significantly linked to EAC (p < 5 × 10−8) were selected, with minimal linkage disequilibrium (R2 < 0.001) to ensure independent effects. Pleiotropic effects were addressed using the PhenoScanner database, and palindromic SNPs were excluded. The inverse variance weighted (IVW) method was the primary approach, with additional MR methods employed. Detailed methods are provided in the supplementary materials.
Results
A comprehensive atlas of risk factors associated with EAC
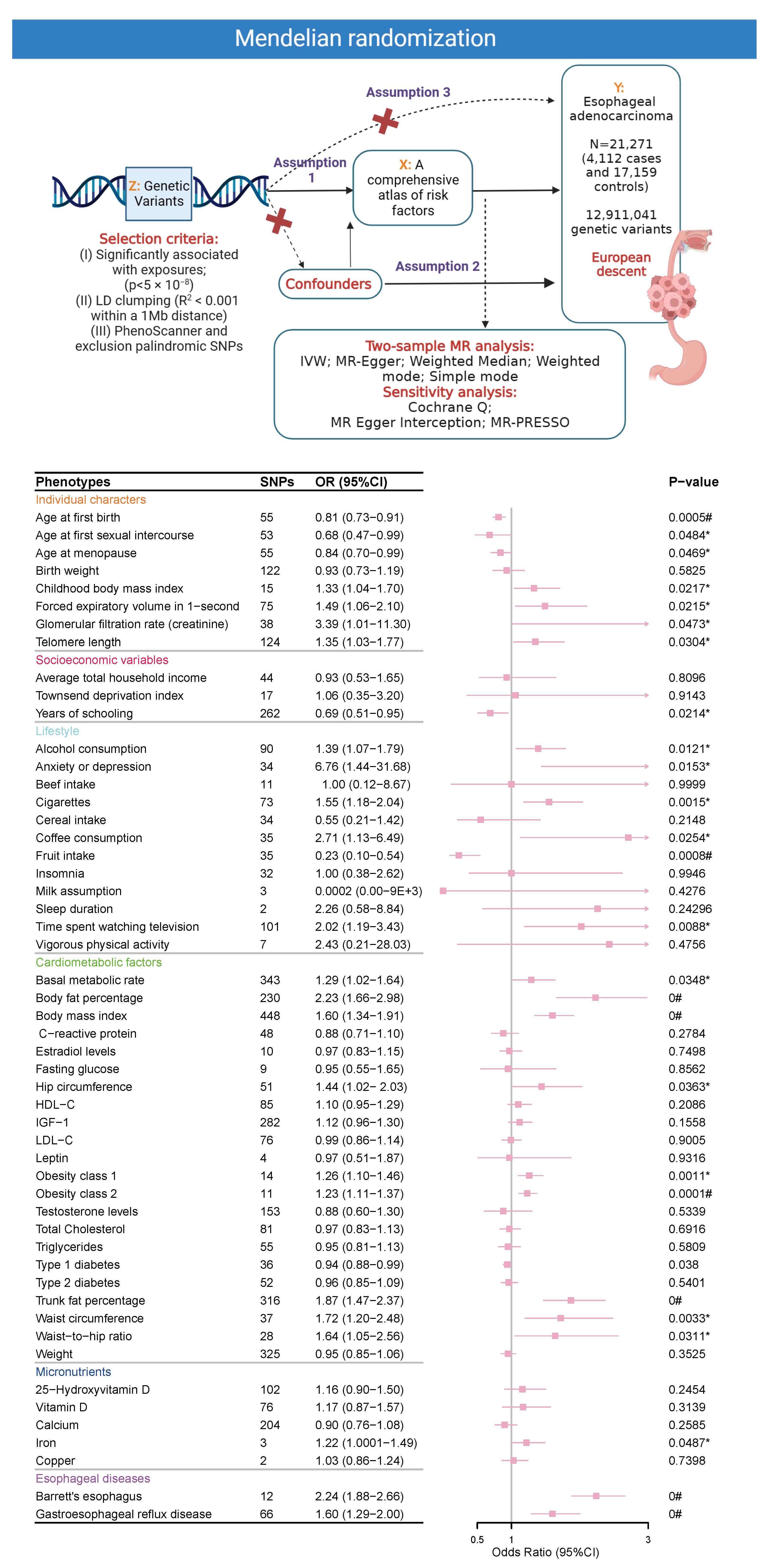
The MR estimates revealed a suggestive or significant relationship between an elevated risk of EAC and 27 key risk and protective factors. Among these, body mass index (OR IVW: 1.6; 95% CI 1.34–1.91, p < 0.001), Barrett’s esophagus (OR IVW: 2.24; 95% CI 1.88–2.66, p < 0.001), and fruit intake (OR IVW: 0.23; 95% CI 0.1–0.54, p < 0.001) stood out as the most critical determinants of risk and protection, respectively. Body mass index, along with obesity traits such as trunk fat percentage (OR IVW: 1.87; 95% CI 1.47–2.37, p < 0.001), waist circumference (OR IVW: 1.72; 95% CI 1.20–2.48, p = 0.003), and waist-to-hip ratio (OR IVW: 1.64; 95% CI 1.05–2.56, p = 0.03), was strongly associated with increased EAC risk, highlighting the role of adiposity in carcinogenesis. In contrast, fruit intake demonstrated significant protective effects, potentially due to its antioxidative and anti-inflammatory properties.
Beyond these major factors, the analysis identified additional modifiable and non-modifiable contributors to EAC risk. Modifiable factors included smoking (OR IVW: 1.55; 95% CI 1.18–2.04, p=0.0015), alcohol consumption (OR IVW: 1.39; 95% CI 1.07–1.79, p=0.01), coffee consumption (OR IVW: 2.71; 95% CI 1.13–6.49, p=0.025), and sedentary behavior as indicated by time spent watching television (OR IVW: 2.02; 95% CI 1.19–3.43, p=0.0088). These factors underscore the importance of lifestyle interventions in mitigating EAC risk. On the other hand, non-modifiable factors such as telomere length (OR IVW: 1.35; 95% CI 1.03–1.77, p=0.03), glomerular filtration rate (OR IVW: 3.39; 95% CI 1.01–11.3, p=0.04), and childhood body mass index (OR IVW: 1.33; 95% CI 1.04–1.7, p=0.02) reflect intrinsic biological and physiological predispositions contributing to EAC risk.
The study also revealed suggestive causal relationships between genetically predicted protective factors and a decreased risk of EAC, including age at first birth (OR IVW: 0.81; 95% CI 0.73–0.91, p=0.0005), age at first sexual intercourse (OR IVW: 0.68; 95% CI 0.47–0.99, p=0.04), age at menarche (OR IVW: 0.84; 95% CI 0.70–0.99, p=0.04), years of schooling (OR IVW: 0.69; 95% CI 0.51–0.95, p=0.02), type 1 diabetes (OR IVW: 0.94; 95% CI 0.88–0.99, p=0.04), and fruit intake (OR IVW: 0.23; 95% CI 0.1–0.54, p=0.0008). Alternative MR methods, including simple mode, weighted mode, weighted median, and MR-Egger regression, yielded consistent results with the IVW findings, supporting the robustness of these conclusions. No evidence of causality was found for other risk factors (all p-values > 0.05) (Figure 1 and Supplementary Table S2).
Figure 1: The overview of the present study depicting a comprehensive atlas of risk factor related to esophageal adenocarcinoma. Within this intricate analysis, genetic variants (Z) assume the crucial role of genetic instruments, enabling an assessment of the causal relationship between exposures (X) and outcomes (Y). The numerical labels 1 to 3 archetypally correspond to assumptions 1 to 3.
Sensitivity analyses
To ensure fidelity of our initial MR discoveries, we have conducted sensitivity analyses that strictly adhere to the three first principles of MR (Figure 1). Table 1 displays the results of these sensitivity analyses. We have identified SNPs that are significantly associated with exposures at a noteworthy p-value threshold (p < 5 x 10-8) and excluded SNPs associated with potential confounders, indicating that the first and third assumptions of MR were not violated. Cochrane’s Q test and MR-Egger intercept regression analyses primarily yielded non-significant p-values (the majority of p-values were greater than 0.05), suggesting an absence of significant heterogeneity and horizontal pleiotropy, respectively (Table 1 ). Furthermore, the MR PRESSO global test identified rs543874, rs429358, rs4627713, rs2041376, rs957919, and rs1516725 as potential sources of pleiotropy (Table 1 ). Previous studies have suggested that multiplicative interactions exist between rs543874[12] , rs429358[6] , and rs1516725[15] with traits such as obesity or apolipoproteins. These findings highlight the importance of cautious interpretation of results involving these SNPs. While the inclusion of these SNPs marginally affected the causal estimate, exclusion analyses yielded consistent results, reinforcing the robustness of our primary findings, suggesting that the potential pleiotropy associated with these SNPs does not substantially undermine the validity of our conclusions.
|
Table 1. Sensitivity analyses. |
||||||||||
|
Phenotypes |
SNPs |
F-value |
Cochrane Q test |
MR Egger Interceotion |
MR PRESSO |
|||||
|
Q |
Q_df |
P-value |
Intercept |
SE |
P-value |
Potential outliers |
global test_P-value |
|||
|
Individual characters |
|
|
|
|
|
|
|
|
|
|
|
Age at first birth |
55.00 |
NA |
50.96 |
54.00 |
0.59 |
0.01 |
0.02 |
0.53 |
NO |
0.61 |
|
Age at first sexual intercourse |
53.00 |
NA |
47.70 |
52.00 |
0.64 |
0.01 |
0.02 |
0.56 |
NO |
0.66 |
|
Age at menopause |
55.00 |
93.04 |
45.79 |
54.00 |
0.78 |
0.01 |
0.02 |
0.58 |
NO |
0.79 |
|
Birth weight |
122.00 |
56.99 |
138.94 |
121.00 |
0.13 |
0.01 |
0.01 |
0.11 |
NO |
0.11 |
|
Childhood body mass index |
15.00 |
NA |
23.60 |
14.00 |
0.05 |
-0.04 |
0.04 |
0.36 |
rs543874 |
0.00 |
|
Forced expiratory volume in 1-second |
75.00 |
46.72 |
126.78 |
74.00 |
0.00 |
-0.04 |
0.02 |
0.07 |
NO |
0.00 |
|
Glomerular filtration rate (creatinine) |
38.00 |
66.38 |
42.60 |
37.00 |
0.24 |
0.01 |
0.02 |
0.61 |
NO |
0.27 |
|
Telomere length |
124.00 |
115.33 |
166.27 |
123.00 |
0.01 |
0.00 |
0.01 |
0.93 |
NO |
0.01 |
|
Socioeconomic variables |
|
|
|
|
|
|
|
|
|
|
|
Average total household income |
44.00 |
40.92 |
60.30 |
43.00 |
0.04 |
-0.01 |
0.02 |
0.61 |
NO |
0.05 |
|
Townsend deprivation index |
17.00 |
35.51 |
21.31 |
16.00 |
0.17 |
0.04 |
0.07 |
0.64 |
NO |
0.17 |
|
Years of schooling |
262.00 |
49.26 |
328.01 |
261.00 |
0.00 |
0.01 |
0.01 |
0.23 |
NO |
0.00 |
|
Lifestyle |
|
|
|
|
|
|
|
|
|
|
|
Alcohol assumption |
90.00 |
53.78 |
99.38 |
89.00 |
0.21 |
0.01 |
0.01 |
0.11 |
NO |
0.21 |
|
Anxiety or depression |
34.00 |
37.20 |
40.59 |
33.00 |
0.17 |
0.02 |
0.04 |
0.61 |
NO |
0.18 |
|
Beef intake |
11.00 |
39.67 |
19.27 |
10.00 |
0.04 |
-0.07 |
0.07 |
0.39 |
rs429358 |
0.00 |
|
Cigarettes |
73.00 |
42.42 |
75.62 |
72.00 |
0.36 |
0.01 |
0.02 |
0.66 |
NO |
0.39 |
|
Cereal intake |
34.00 |
45.50 |
49.12 |
33.00 |
0.04 |
0.02 |
0.03 |
0.47 |
NO |
0.05 |
|
Coffee consumed |
35.00 |
77.66 |
57.96 |
34.00 |
0.01 |
0.00 |
0.01 |
0.90 |
NO |
0.01 |
|
Fruit intake |
35.00 |
40.36 |
41.17 |
34.00 |
0.19 |
-0.02 |
0.03 |
0.54 |
NO |
0.20 |
|
Insomnia |
32.00 |
45.46 |
42.21 |
31.00 |
0.09 |
0.03 |
0.02 |
0.17 |
NO |
0.10 |
|
Milk assumption |
3.00 |
38.17 |
6.09 |
2.00 |
0.05 |
-0.03 |
0.29 |
0.93 |
NO |
NA |
|
Sleep duration |
2.00 |
49.45 |
NA |
NA |
NA |
NA |
NA |
NA |
NO |
NA |
|
Time spent watching television |
101.00 |
41.41 |
114.91 |
100.00 |
0.15 |
-0.01 |
0.02 |
0.71 |
NO |
0.15 |
|
Vigorous physical activity |
7.00 |
40.81 |
5.35 |
6.00 |
0.50 |
0.04 |
0.10 |
0.71 |
NO |
0.53 |
|
Cardiometabolic factors |
|
|
|
|
|
|
|
|
|
|
|
Basal metabolic rate |
343.00 |
70.37 |
407.23 |
342.00 |
0.01 |
0.00 |
0.00 |
0.47 |
rs4627713 |
0.00 |
|
Body fat percentage |
230.00 |
51.95 |
274.91 |
229.00 |
0.02 |
-0.01 |
0.01 |
0.35 |
rs2041376 |
0.00 |
|
Body mass index |
448.00 |
71.65 |
493.32 |
447.00 |
0.06 |
-0.01 |
0.00 |
0.19 |
NO |
0.07 |
|
C-reactive protein |
48.00 |
128.08 |
67.05 |
47.00 |
0.03 |
0.00 |
0.01 |
0.95 |
NO |
0.03 |
|
Estradiol levels |
10.00 |
67.65 |
11.28 |
9.00 |
0.26 |
0.02 |
0.04 |
0.60 |
NO |
0.34 |
|
Fasting glucose |
9.00 |
NA |
10.42 |
8.00 |
0.24 |
0.02 |
0.03 |
0.45 |
NO |
0.29 |
|
Hip circumference |
51.00 |
55.29 |
73.86 |
50.00 |
0.02 |
-0.04 |
0.01 |
0.02 |
rs4889606 |
0.00 |
|
HDL-C |
85.00 |
121.06 |
89.75 |
84.00 |
0.31 |
0.00 |
0.01 |
0.60 |
NO |
0.32 |
|
IGF-1 |
282.00 |
101.83 |
334.61 |
281.00 |
0.02 |
0.00 |
0.00 |
0.44 |
NO |
0.01 |
|
LDL-C |
76.00 |
158.18 |
98.38 |
75.00 |
0.04 |
0.00 |
0.01 |
0.86 |
NO |
0.04 |
|
Leptin |
4.00 |
39.68 |
3.70 |
3.00 |
0.30 |
0.00 |
0.11 |
0.97 |
rs4731702 |
0.01 |
|
Obesity class 1 |
14.00 |
67.39 |
16.13 |
13.00 |
0.24 |
-0.04 |
0.02 |
0.08 |
NO |
0.25 |
|
Obesity class 2 |
11.00 |
61.46 |
16.98 |
10.00 |
0.07 |
-0.08 |
0.03 |
0.02 |
NO |
0.11 |
|
Testosterone levels |
153.00 |
81.61 |
173.66 |
152.00 |
0.11 |
0.00 |
0.01 |
0.95 |
NO |
0.11 |
|
Total Cholesterol |
81.00 |
137.98 |
110.12 |
80.00 |
0.01 |
0.00 |
0.01 |
0.59 |
NO |
0.02 |
|
Triglycerides |
55.00 |
169.89 |
65.97 |
54.00 |
0.13 |
0.01 |
0.01 |
0.38 |
NO |
0.15 |
|
Type 1 diabetes |
36.00 |
NA |
51.72 |
35.00 |
0.03 |
-0.01 |
0.01 |
0.24 |
NO |
0.04 |
|
Type 2 diabetes |
52.00 |
NA |
60.56 |
51.00 |
0.17 |
0.01 |
0.01 |
0.47 |
NO |
0.19 |
|
Trunk fat percentage |
316.00 |
59.17 |
388.99 |
315.00 |
0.00 |
-0.01 |
0.01 |
0.22 |
rs957919 |
0.00 |
|
Waist circumference |
37.00 |
50.57 |
48.35 |
36.00 |
0.08 |
-0.03 |
0.02 |
0.14 |
rs1516725 |
0.01 |
|
Waist-to-hip ratio |
28.00 |
45.42 |
27.78 |
27.00 |
0.42 |
-0.04 |
0.03 |
0.14 |
NO |
0.40 |
|
Weight |
325.00 |
79.19 |
320.78 |
324.00 |
0.54 |
0.00 |
0.00 |
0.60 |
NO |
0.55 |
|
Micronutrients |
|
|
|
|
|
|
|
|
|
|
|
25-Hydroxyvitamin D |
102.00 |
113.03 |
122.41 |
101.00 |
0.07 |
0.01 |
0.01 |
0.03 |
NO |
0.07 |
|
Vitamin D |
76.00 |
133.61 |
97.70 |
75.00 |
0.04 |
0.00 |
0.01 |
0.50 |
NO |
0.05 |
|
Calcium |
204.00 |
101.29 |
214.01 |
203.00 |
0.28 |
0.00 |
0.00 |
0.29 |
NO |
0.30 |
|
Iron |
3.00 |
NA |
0.83 |
2.00 |
0.66 |
0.02 |
0.04 |
0.68 |
NO |
NA |
|
Copper |
2.00 |
NA |
NA |
NA |
NA |
NA |
NA |
NA |
NO |
NA |
|
Esophageal diseases |
|
|
|
|
|
|
|
|
|
|
|
Barrett's esophagus |
12.00 |
35.88 |
16.82 |
11.00 |
0.11 |
0.02 |
0.07 |
0.79 |
NO |
0.24 |
|
Gastroesophageal reflux disease |
66.00 |
38.95 |
80.79 |
65.00 |
0.09 |
-0.02 |
0.02 |
0.33 |
NO |
0.09 |
Discussion
To the best of our knowledge, this study represents a novel and comprehensive examination of latent and modifiable risk factors associated with EAC. Beyond the established risk factors such as alcohol consumption, smoking, Barrett’s esophagus, and gastroesophageal reflux disease, our findings provide insights into previously underexplored dimensions of EAC risk, offering a more nuanced understanding of its etiology. Of note, the progression from Barrett’s esophagus to EAC is driven by a series of molecular and cellular changes that result in dysregulated cell growth, altered gene expression, and increased resistance to apoptosis. One of the key events in this process is the accumulation of genetic mutations that facilitate carcinogenesis. Mutations in tumor suppressor genes, such as TP53, and the amplification of oncogenes like c-MYC and cyclin D1, have been frequently observed in the transition from Barrett’s esophagus to EAC [17,18] . These genetic alterations contribute to the loss of normal growth control, allowing abnormal cells to proliferate uncontrollably and form a tumor. Moreover, smoking induces chronic inflammation and DNA damage through the generation of reactive oxygen species, while alcohol enhances acetaldehyde production, further promoting mutagenesis.
In the present study, we have identified several factors related to individual characteristics that may either protect or increase the risk of EAC. These factors include age at first birth, age at first sexual intercourse, age at menarche, birth weight, forced expiratory volume in 1-second, glomerular filtration rate, and telomere length. We also confirmed associations previously suggested by other studies, such as the link between reproductive factors [14] and telomere length [23] with cancer. However, our study is the first to establish these associations with EAC specifically. Additionally, our study uniquely identifies lung and kidney function as potential risk factors for EAC, suggesting that systemic physiological health may influence esophageal carcinogenesis. Reduced forced expiratory volume in one second may reflect compromised respiratory function and chronic exposure to oxidative stress or inflammation, which could contribute to cancer risk. Similarly, impaired glomerular filtration rate, indicative of kidney dysfunction, could be linked to an altered metabolic profile, systemic inflammation, or impaired clearance of carcinogenic compounds, all of which may play a role in EAC development [13] .
Our study has identified several modifiable risk factors that contribute to an increased risk of EAC. These include habits like alcohol consumption, smoking, coffee consumption, and sedentary behavior (measured by television viewing duration). On the other hand, fruit consumption exhibited a potentially protective effect against the development of EAC. Fruit consumption exhibits a protective effect against EAC are consistent with prior studies that have emphasized the role of diet in cancer prevention. Mechanistically, fruits are rich sources of antioxidants, such as vitamins C and E, flavonoids, and carotenoids, which can neutralize reactive oxygen species and reduce oxidative stress—a key driver of carcinogenesis[8,21] . Additionally, fruits contain anti-inflammatory compounds that may mitigate chronic inflammation, a well-recognized precursor to EAC development. For instance, polyphenols in fruits have been shown to downregulate pro-inflammatory pathways, such as NF-κB signaling, which is frequently activated in EAC[3] . Furthermore, dietary fiber found in fruits contributes to gut microbiome health, promoting the production of short-chain fatty acids that exhibit anti-tumorigenic properties[22] . These multifaceted benefits underscore the biological plausibility of the protective role of fruit consumption in EAC prevention.
Moreover, our findings have not only confirmed previous large-scale cohort studies linking obesity to a significant increase in esophageal and gastric cancer incidence[1] , but have also expanded upon these findings by establishing links between specific obesity traits (such as obesity class 1 and 2, trunk fat percentage, waist circumference, and waist-to-hip ratio) and an elevated risk of EAC. Obesity has long been recognized as an important factor in the pathogenesis of various cancers, including EAC, colorectal cancer, breast cancer, and endometrial cancer. The relationship between BMI and cancer is multifactorial, involving complex mechanisms such as chronic low-grade inflammation, hormonal dysregulation, and altered metabolic processes. One of the primary mechanisms through which obesity contributes to cancer risk is the pro-inflammatory state induced by excess adipose tissue. Adipocytes secrete a variety of pro-inflammatory cytokines, including interleukins, tumor necrosis factor-alpha, and leptin, which can promote chronic inflammation[1,10] . This chronic inflammatory environment facilitates cellular mutations, tumor initiation, and progression. These observations underscore the critical role of fat distribution and central obesity, beyond generalized body mass index, in influencing cancer susceptibility, likely through mechanisms involving systemic inflammation, hormonal dysregulation, and altered metabolic profiles. Additionally, we have identified a causal relationship between genetically predicted risk of EAC and type 1 diabetes, as well as serum iron levels. Elevated serum iron levels could exacerbate oxidative stress through the Fenton reaction, generating reactive oxygen species that damage DNA, proteins, and lipids[9,16] . Conversely, dysregulated iron homeostasis might impair cellular energy metabolism and immune responses, further promoting tumor initiation and progression[16] . These findings provide a compelling rationale for exploring iron modulation as a potential therapeutic or preventative strategy in high-risk populations.
Our work sheds light on a comprehensive range of risk factors associated with EAC. While these findings significantly contribute to understanding the etiology of EAC, several limitations must be acknowledged. First, in our present study, the participants analyzed were of European ancestry. Our findings for specific cancers might lack validation using multiple datasets. Consequently, caution must be exercised when extrapolating these findings to other populations, as it may introduce bias and limit the generalizability of the results. Additionally, despite employing robust statistical methods, such as MR Egger intercept tests, MR PRESSO global tests, and Cochran’s Q tests, to identify and mitigate the effects of pleiotropy, it is not possible to entirely rule out residual pleiotropy in our analysis. Certain SNPs, such as rs429358 and rs543874, were identified as potential sources of pleiotropic effects, given their known associations with multiple phenotypes beyond the primary exposures studied. These findings emphasize the need for cautious interpretation of causal estimates, particularly for associations involving these SNPs. Further functional validation and investigations in diverse populations are necessary to confirm and extend our findings. Nonetheless, these results provide a valuable foundation for preventive measures, early detection, and targeted interventions to reduce the incidence of this disease.
Conclusion
Our work is to shed light on a comprehensive range of risk factors associated with EAC. These findings contribute to our understanding of the etiology of EAC and may have implications for preventive measures, early detection, and targeted interventions to reduce the incidence of this disease.[5]
Abbreviations
EAC: Esophageal adenocarcinoma, CI: confidence interval, GWAS: genome-wide association studies, IVs: genetic instruments, IVW: Inverse variance weighted, LD: linkage disequilibrium, MR: Mendelian randomization, OR: odds ratio, SNPs: single nucleotide polymorphisms.
Supplementary Material
Supplementary methods, results, spectra, figures.
Acknowledgements
We appreciate the work of the open GWAS project (https://gwas.mrcieu.ac.uk/).
Author contributions
Wenjie Li: Conceptualization, methodology, data curation, software and writing-review & editing, project administration, supervision and validation. The work reported in the paper has been performed by the authors, unless clearly specified in the text.
Ethics approval and consent to participate
No ethics approval and written consent were needed for the secondary analysis of public data.
Funding information
None.
Competing Interests
The authors declare that they have no existing or potential commercial or financial relationships that could create a conflict of interest at the time of conducting this study.
Data Availability
All data needed to evaluate the conclusions in the paper are present in the paper or the Supplementary Materials. Additional data related to this paper may be requested from the authors.
References
[1] Avgerinos, K. I., Spyrou, N., Mantzoros, C. S., & Dalamaga, M. (2019, Mar). Obesity and cancer risk: Emerging biological mechanisms and perspectives. Metabolism, 92, 121-135. https://doi.org/10.1016/j.metabol.2018.11.001
[2] Burgess, S., & Labrecque, J. (2018). Mendelian randomization with a binary exposure variable: interpretation and presentation of causal estimates. European journal of epidemiology, 33(10), 947-952. https://doi.org/10.1007/s10654-018-0424-6
[3] Chen, L., Lu, H., Peng, D., Cao, L. L., Ballout, F., Srirmajayam, K., et al. (2023, Mar). Activation of NOTCH signaling via DLL1 is mediated by APE1-redox-dependent NF-κB activation in oesophageal adenocarcinoma. Gut, 72(3), 421-432. https://doi.org/10.1136/gutjnl-2022-327076
[4] Coleman, H. G., Xie, S.-H., & Lagergren, J. (2018, 2018/1//). The Epidemiology of Esophageal Adenocarcinoma. Gastroenterology, 154(2), 390-405. https://doi.org/10.1053/j.gastro.2017.07.046
[5] Global Burden of Disease Cancer, C., Kocarnik, J. M., Compton, K., Dean, F. E., Fu, W., Gaw, B. L., et al. (2022, 2022/3/1/). Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life Years for 29 Cancer Groups From 2010 to 2019: A Systematic Analysis for the Global Burden of Disease Study 2019. JAMA oncology, 8(3), 420-444. https://doi.org/10.1001/jamaoncol.2021.6987
[6] Innes, H., Nischalke, H. D., Guha, I. N., Weiss, K. H., Irving, W., Gotthardt, D., et al. (2022, May). The rs429358 Locus in Apolipoprotein E Is Associated With Hepatocellular Carcinoma in Patients With Cirrhosis. Hepatol Commun, 6(5), 1213-1226. https://doi.org/10.1002/hep4.1886
[7] Joseph, A., Raja, S., Kamath, S., Jang, S., Allende, D., McNamara, M., et al. (2022, May 2). Esophageal adenocarcinoma: A dire need for early detection and treatment. Cleve Clin J Med, 89(5), 269-279. https://doi.org/10.3949/ccjm.89a.21053
[8] Kashif, M., Yao, H., Schmidt, S., Chen, X., Truong, M., Tüksammel, E., et al. (2023, Apr). ROS-lowering doses of vitamins C and A accelerate malignant melanoma metastasis. Redox Biol, 60, 102619. https://doi.org/10.1016/j.redox.2023.102619
[9] Kawabata, T. (2022, Jul 8). Iron-Induced Oxidative Stress in Human Diseases. Cells, 11(14). https://doi.org/10.3390/cells11142152
[10] Lega, I. C., & Lipscombe, L. L. (2020, Feb 1). Review: Diabetes, Obesity, and Cancer-Pathophysiology and Clinical Implications. Endocr Rev, 41(1). https://doi.org/10.1210/endrev/bnz014
[11] Li, W., Wang, R., & Wang, W. (2022). Exploring the causality and pathogenesis of systemic lupus erythematosus in breast cancer based on Mendelian randomization and transcriptome data analyses. Front Immunol, 13, 1029884. https://doi.org/10.3389/fimmu.2022.1029884
[12] Mei, H., Yin, B., Yang, W., Zhang, J., Lu, H., Qi, X., et al. (2022). Associations between Gene-Gene Interaction and Overweight/Obesity of 12-Month-Old Chinese Infants. Biomed Res Int, 2022, 1499454. https://doi.org/10.1155/2022/1499454
[13] Nøst, T. H., Alcala, K., Urbarova, I., Byrne, K. S., Guida, F., Sandanger, T. M., et al. (2021, Aug). Systemic inflammation markers and cancer incidence in the UK Biobank. Eur J Epidemiol, 36(8), 841-848. https://doi.org/10.1007/s10654-021-00752-6
[14] Peng, H., Wu, X., Wen, Y., Du, X., Li, C., Liang, H., et al. (2021, 2021/4//). Age at first birth and lung cancer: a two-sample Mendelian randomization study. Translational lung cancer research, 10(4), 1720-1733. https://doi.org/10.21037/tlcr-20-1216
[15] Pisanu, C., Williams, M. J., Ciuculete, D. M., Olivo, G., Del Zompo, M., Squassina, A., et al. (2019, Nov 21). Evidence that genes involved in hedgehog signaling are associated with both bipolar disorder and high BMI. Transl Psychiatry, 9(1), 315. https://doi.org/10.1038/s41398-019-0652-x
[16] Qin, M., Shao, B., Lin, L., Zhang, Z. Q., Sheng, Z. G., Qin, L., et al. (2023, Jan). Molecular mechanism of the unusual biphasic effects of the natural compound hinokitiol on iron-induced cellular DNA damage. Free Radic Biol Med, 194, 163-171. https://doi.org/10.1016/j.freeradbiomed.2022.11.042
[17] Rajendra, S., Sharma, P., Gautam, S. D., Saxena, M., Kapur, A., Sharma, P., et al. (2020, Feb 5). Association of Biomarkers for Human Papillomavirus With Survival Among Adults With Barrett High-grade Dysplasia and Esophageal Adenocarcinoma. JAMA Netw Open, 3(2), e1921189. https://doi.org/10.1001/jamanetworkopen.2019.21189
[18] Redston, M., Noffsinger, A., Kim, A., Akarca, F. G., Rara, M., Stapleton, D., et al. (2022, Feb). Abnormal TP53 Predicts Risk of Progression in Patients With Barrett's Esophagus Regardless of a Diagnosis of Dysplasia. Gastroenterology, 162(2), 468-481. https://doi.org/10.1053/j.gastro.2021.10.038
[19] Sekula, P., Del Greco M, F., Pattaro, C., & Köttgen, A. (2016, 2016/11//). Mendelian Randomization as an Approach to Assess Causality Using Observational Data. Journal of the American Society of Nephrology, 27(11), 3253-3265. https://doi.org/10.1681/ASN.2016010098
[20] Siegel, R. L., Miller, K. D., & Jemal, A. (2020, Jan). Cancer statistics, 2020. CA Cancer J Clin, 70(1), 7-30. https://doi.org/10.3322/caac.21590
[21] Su, X., Shen, Z., Yang, Q., Sui, F., Pu, J., Ma, J., et al. (2019). Vitamin C kills thyroid cancer cells through ROS-dependent inhibition of MAPK/ERK and PI3K/AKT pathways via distinct mechanisms. Theranostics, 9(15), 4461-4473. https://doi.org/10.7150/thno.35219
[22] Tanes, C., Bittinger, K., Gao, Y., Friedman, E. S., Nessel, L., Paladhi, U. R., et al. (2021, Mar 10). Role of dietary fiber in the recovery of the human gut microbiome and its metabolome. Cell Host Microbe, 29(3), 394-407.e395. https://doi.org/10.1016/j.chom.2020.12.012
[23] Telomeres Mendelian Randomization, C., Haycock, P. C., Burgess, S., Nounu, A., Zheng, J., Okoli, G. N., et al. (2017, 2017/5/1/). Association Between Telomere Length and Risk of Cancer and Non-Neoplastic Diseases: A Mendelian Randomization Study. JAMA oncology, 3(5), 636-651. https://doi.org/10.1001/jamaoncol.2016.5945
 Figures
Figures References
References Peer
Peer Information
InformationFigure 1: The overview of the present study depicting a comprehensive atlas of risk factor related to esophageal adenocarcinoma. Within this intricate analysis, genetic variants (Z) assume the crucial role of genetic instruments, enabling an assessment of the causal relationship between exposures (X) and outcomes (Y). The numerical labels 1 to 3 archetypally correspond to assumptions 1 to 3.
[1] Avgerinos, K. I., Spyrou, N., Mantzoros, C. S., & Dalamaga, M. (2019, Mar). Obesity and cancer risk: Emerging biological mechanisms and perspectives. Metabolism, 92, 121-135. https://doi.org/10.1016/j.metabol.2018.11.001
[2] Burgess, S., & Labrecque, J. (2018). Mendelian randomization with a binary exposure variable: interpretation and presentation of causal estimates. European journal of epidemiology, 33(10), 947-952. https://doi.org/10.1007/s10654-018-0424-6
[3] Chen, L., Lu, H., Peng, D., Cao, L. L., Ballout, F., Srirmajayam, K., et al. (2023, Mar). Activation of NOTCH signaling via DLL1 is mediated by APE1-redox-dependent NF-κB activation in oesophageal adenocarcinoma. Gut, 72(3), 421-432. https://doi.org/10.1136/gutjnl-2022-327076
[4] Coleman, H. G., Xie, S.-H., & Lagergren, J. (2018, 2018/1//). The Epidemiology of Esophageal Adenocarcinoma. Gastroenterology, 154(2), 390-405. https://doi.org/10.1053/j.gastro.2017.07.046
[5] Global Burden of Disease Cancer, C., Kocarnik, J. M., Compton, K., Dean, F. E., Fu, W., Gaw, B. L., et al. (2022, 2022/3/1/). Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life Years for 29 Cancer Groups From 2010 to 2019: A Systematic Analysis for the Global Burden of Disease Study 2019. JAMA oncology, 8(3), 420-444. https://doi.org/10.1001/jamaoncol.2021.6987
[6] Innes, H., Nischalke, H. D., Guha, I. N., Weiss, K. H., Irving, W., Gotthardt, D., et al. (2022, May). The rs429358 Locus in Apolipoprotein E Is Associated With Hepatocellular Carcinoma in Patients With Cirrhosis. Hepatol Commun, 6(5), 1213-1226. https://doi.org/10.1002/hep4.1886
[7] Joseph, A., Raja, S., Kamath, S., Jang, S., Allende, D., McNamara, M., et al. (2022, May 2). Esophageal adenocarcinoma: A dire need for early detection and treatment. Cleve Clin J Med, 89(5), 269-279. https://doi.org/10.3949/ccjm.89a.21053
[8] Kashif, M., Yao, H., Schmidt, S., Chen, X., Truong, M., Tüksammel, E., et al. (2023, Apr). ROS-lowering doses of vitamins C and A accelerate malignant melanoma metastasis. Redox Biol, 60, 102619. https://doi.org/10.1016/j.redox.2023.102619
[9] Kawabata, T. (2022, Jul 8). Iron-Induced Oxidative Stress in Human Diseases. Cells, 11(14). https://doi.org/10.3390/cells11142152
[10] Lega, I. C., & Lipscombe, L. L. (2020, Feb 1). Review: Diabetes, Obesity, and Cancer-Pathophysiology and Clinical Implications. Endocr Rev, 41(1). https://doi.org/10.1210/endrev/bnz014
[11] Li, W., Wang, R., & Wang, W. (2022). Exploring the causality and pathogenesis of systemic lupus erythematosus in breast cancer based on Mendelian randomization and transcriptome data analyses. Front Immunol, 13, 1029884. https://doi.org/10.3389/fimmu.2022.1029884
[12] Mei, H., Yin, B., Yang, W., Zhang, J., Lu, H., Qi, X., et al. (2022). Associations between Gene-Gene Interaction and Overweight/Obesity of 12-Month-Old Chinese Infants. Biomed Res Int, 2022, 1499454. https://doi.org/10.1155/2022/1499454
[13] Nøst, T. H., Alcala, K., Urbarova, I., Byrne, K. S., Guida, F., Sandanger, T. M., et al. (2021, Aug). Systemic inflammation markers and cancer incidence in the UK Biobank. Eur J Epidemiol, 36(8), 841-848. https://doi.org/10.1007/s10654-021-00752-6
[14] Peng, H., Wu, X., Wen, Y., Du, X., Li, C., Liang, H., et al. (2021, 2021/4//). Age at first birth and lung cancer: a two-sample Mendelian randomization study. Translational lung cancer research, 10(4), 1720-1733. https://doi.org/10.21037/tlcr-20-1216
[15] Pisanu, C., Williams, M. J., Ciuculete, D. M., Olivo, G., Del Zompo, M., Squassina, A., et al. (2019, Nov 21). Evidence that genes involved in hedgehog signaling are associated with both bipolar disorder and high BMI. Transl Psychiatry, 9(1), 315. https://doi.org/10.1038/s41398-019-0652-x
[16] Qin, M., Shao, B., Lin, L., Zhang, Z. Q., Sheng, Z. G., Qin, L., et al. (2023, Jan). Molecular mechanism of the unusual biphasic effects of the natural compound hinokitiol on iron-induced cellular DNA damage. Free Radic Biol Med, 194, 163-171. https://doi.org/10.1016/j.freeradbiomed.2022.11.042
[17] Rajendra, S., Sharma, P., Gautam, S. D., Saxena, M., Kapur, A., Sharma, P., et al. (2020, Feb 5). Association of Biomarkers for Human Papillomavirus With Survival Among Adults With Barrett High-grade Dysplasia and Esophageal Adenocarcinoma. JAMA Netw Open, 3(2), e1921189. https://doi.org/10.1001/jamanetworkopen.2019.21189
[18] Redston, M., Noffsinger, A., Kim, A., Akarca, F. G., Rara, M., Stapleton, D., et al. (2022, Feb). Abnormal TP53 Predicts Risk of Progression in Patients With Barrett's Esophagus Regardless of a Diagnosis of Dysplasia. Gastroenterology, 162(2), 468-481. https://doi.org/10.1053/j.gastro.2021.10.038
[19] Sekula, P., Del Greco M, F., Pattaro, C., & Köttgen, A. (2016, 2016/11//). Mendelian Randomization as an Approach to Assess Causality Using Observational Data. Journal of the American Society of Nephrology, 27(11), 3253-3265. https://doi.org/10.1681/ASN.2016010098
[20] Siegel, R. L., Miller, K. D., & Jemal, A. (2020, Jan). Cancer statistics, 2020. CA Cancer J Clin, 70(1), 7-30. https://doi.org/10.3322/caac.21590
[21] Su, X., Shen, Z., Yang, Q., Sui, F., Pu, J., Ma, J., et al. (2019). Vitamin C kills thyroid cancer cells through ROS-dependent inhibition of MAPK/ERK and PI3K/AKT pathways via distinct mechanisms. Theranostics, 9(15), 4461-4473. https://doi.org/10.7150/thno.35219
[22] Tanes, C., Bittinger, K., Gao, Y., Friedman, E. S., Nessel, L., Paladhi, U. R., et al. (2021, Mar 10). Role of dietary fiber in the recovery of the human gut microbiome and its metabolome. Cell Host Microbe, 29(3), 394-407.e395. https://doi.org/10.1016/j.chom.2020.12.012
[23] Telomeres Mendelian Randomization, C., Haycock, P. C., Burgess, S., Nounu, A., Zheng, J., Okoli, G. N., et al. (2017, 2017/5/1/). Association Between Telomere Length and Risk of Cancer and Non-Neoplastic Diseases: A Mendelian Randomization Study. JAMA oncology, 3(5), 636-651. https://doi.org/10.1001/jamaoncol.2016.5945
Peer-review Terminology
Identity transparency: Single anonymized
Reviewer interacts with: Editor
Details
This is an open access article under the terms of the Creative Commons Attribution License(http://creativecommons.org/licenses/by/4.0/), which permits use, distribution and reproduction in any medium, provided the original work is properly cited.
Publication History
Received 2025-01-25
Accepted 2025-03-27
Published 2025-03-30